Figure 7.1
X-ray demonstrating tooth fragments adjacent to laceration
Various levels of the root can also be fractured. This should be suspected when the tooth is loose and should be confirmed with an X-ray. If the root tip is fractured, the tooth should be splinted and advice given to contact a dentist. Prescribe analgesics and antibiotics.
Luxated (partially displaced) tooth (Fig. 7.2) should be reduced and splinted. X-rays should be taken to rule out fracture of the root. Advice patients to contact dentist ASAP.
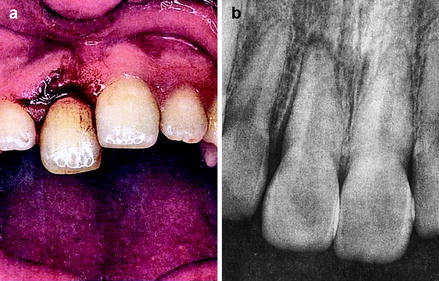
Figure 7.2
Luxated tooth and X-ray excluded fracture of the root
Avulsed teeth (out of the socket) needs rapid treatment. Tooth is best stored in cold milk or patients own mouth until it is reimplanted. Wash with cold running saline and hold it with the crown.
If a whole dentoalveolar segment is fractured, the whole segment has to be reduced and splinted. Any associated gingival tear should be sutured. Impressions can be taken to guide the reduction of teeth and also useful to make a custom-made splint.
Clinical Case Scenario 2: Dental Infection
Case Presentation
A 14-year-old patient presents with a 6-day history of swelling in his left cheek. It was preceded by toothache and is now progressively getting worse. On arrival, he is apyrexial and otherwise well, but looks flushed. He was unable to attend for PE lesson today and his mother took him to the dentist, who immediately referred him to the on call ENT team.
Key Features in History and Examination
History
Ask for duration, source of infection, tooth pain, difficulty in breathing, or swallowing. Ask about diabetes and immunodepression. Previous dental history and imaging taken.
Examination
Assess the extent of the swelling (determine which dental space is involved). Look out for the source of infection (skin, teeth, etc.). Grave signs include trismus, raised floor of mouth, unable to swallow, and drooling of saliva.
Principles of Acute Management
If airway is potentially compromised, one needs urgent airway management. Inform anesthetist for assessment. Try to avoid a tracheostomy. Steroids can be given to reduce edema.
Appropriate antibiotics should be given immediately (to cover cocci and anaerobes). Necessary radiographs (Fig. 7.3) should be taken to identify the source. Drainage is indicated if there is collection of pus. At the same time, the source of infection should be dealt with (e.g. extraction).

Figure 7.3
Orthopantomogram (OPG) showing source of infection
Blood tests should be done to rule out undiagnosed diabetes or other hematological conditions (leukemia).
Discussion
Acute facial swelling due to dental infection can be life threatening. It can progress rapidly in some cases. Therefore, urgent management is critical. In early stages, oral antibiotics are enough with urgent attention to the source of infection. In severe cases, urgent admission for IV antibiotics is important. Continuous monitoring of progress or airway compromise is necessary till the time of definitive management. If there is pus collection, drainage at the earliest is necessary with removal of the source of infection. Depending on the teeth, various spaces can be involved. These include:
1.
Canine space
2.
Buccal space
3.
Submandibular space
4.
Submental space
5.
Sublingual space
6.
Submasseteric space
7.
Pterygomandibular space
8.
Parapharyngeal space
9.
Temporal space
Ludwigs Angina
Ludwig’s angina is an acute and potentially life-threatening cellulitis involving, sublingual, submental, and submandibular spaces often due to dental infection. The tongue is swollen, floor of mouth is raised, and the patient will have difficulty in swallowing (Fig. 7.4). This will lead to airway obstruction if not intervened early. This condition therefore needs immediate management of airway and drainage of the above spaces. Admission to ITU may be necessary. General principles of dental infection management as above apply, but urgent attention to airway and drainage is critical.

Figure 7.4
Image of patient with Ludwig’s angina
Clinical Case Scenario 3: Mandibular Fractures
Case Presentation
A 25-year-old male comes to accident and emergency department with pain and difficulty in closing the mouth after a fight in a nightclub. He was punched once after he insulted his friend’s partner. There was no loss of consciousness and he remembers the incident vividly.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


