CHAPTER 145
Marine Envenomations
Presentation
After swimming in the ocean and coming into contact with marine life, the patient may seek medical attention because of local pain, swelling, or skin discoloration. Marine animal envenomations can be divided into two major categories: puncture wounds and focal rashes. Severe envenomations can be accompanied by systemic symptoms, such as vomiting, paralysis, seizures, respiratory distress, and hypotension. This review is limited to the more common injuries with minor local reactions.
Puncture Wounds
A laceration or puncture wound of the leg with blue edges suggests a stingray attack. There is immediate local intense pain, edema of soft tissue, and a variable amount of bleeding. The pain is excruciating and seems out of proportion to what might be expected based on the wound appearance alone. The pain usually peaks after 60 to 90 minutes, may radiate centrally, generally resolves over several hours, and may last as long as 48 hours. Retained fragments of the stingray’s barb may be present in the wound.
A single small ischemic (e.g., pallor and cyanosis) puncture wound with a red halo and rapid swelling suggests a lionfish or scorpion fish envenomation. The pain is immediate, intense, and radiating. Untreated, the pain peaks 60 to 90 minutes after the sting, persists for at least 6 to 12 hours, and sometimes lasts for days. The severity of envenomations seems to be mild for lionfish, more severe for scorpion fish, and most severe or even life-threatening for stonefish, which is another member of the Scorpaenidae.
The dorsal or pectoral fin spines of the catfish can often inflict an envenomation when puncturing the skin. Symptoms include intense pain, paresthesias, and numbness that may last 30 minutes to 48 hours. Erythema, hemorrhage, edema, cyanosis, and lymphangitis also are common localized findings. Catfish have retroussé barbs (tip turned up) and can produce significant damage and be difficult to remove (Figure 145-1).

Figure 145-1 Catfish spine impalement.
Multiple small punctures in an erratic pattern, with or without purple discoloration, or retained fragments are typical of sea urchin envenomations. The venomous spines can inflict burning pain that is initially minor but intensifies over 30 minutes and lasts several hours. The area surrounding the puncture wounds may be red and swollen. Some spines contain a blue-black dye that stains the wound or causes temporary tattooing.
Focal Rashes
An intense red, itchy rash follows contact with a bristle worm.
Contact with feather hydroids and sea anemones induces a mild reaction, consisting of instantaneous burning, itching, and urticaria. Envenomation may result in a lesion with a pale center and an erythematous or petechial ring; this is followed by increasing edema and ecchymosis. Although most lesions resolve in 48 hours, more severe envenomations may result in vesicle formation, which can lead to an abscess, eschar, or hyperpigmentation.
The sting of the fire coral induces intense burning pain, redness, itching, and painful pruritus with large wheals, with central radiation and reactive regional lymphadenopathy. Fire coral (not a true coral) has a razor-sharp lime carbonate exoskeleton that can cause skin lacerations containing exoskeleton debris.
Envenomation from a jellyfish causes immediate pain that may be described as mild to moderate stinging or burning. Pain is followed by the development of an erythematous rash.
Most jellyfish with suspended tentacles create “tentacle prints” or a whiplike pattern of darkened reddish-brown, purple, or frosted and crosshatched stripes in the precise areas of skin contact (Figure 145-2). Vesiculation and skin necrosis may follow and can last 24 hours or longer. Occasionally, there will be residual hyperpigmentation. Tentacles still may be adherent on patient presentation.
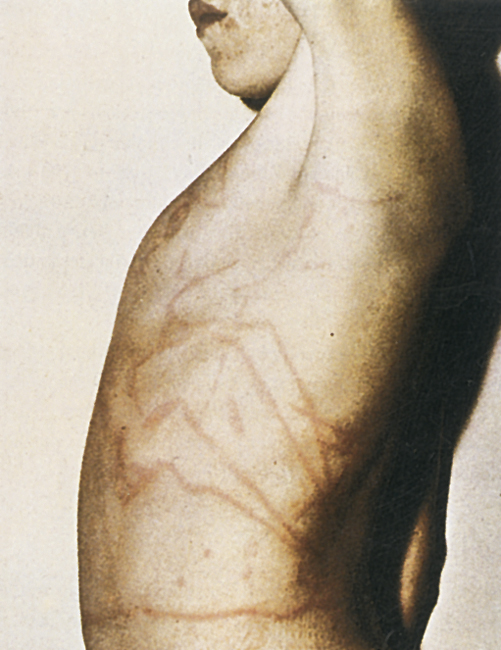
Figure 145-2 “Tentacle prints” from the Atlantic Portuguese man-of-war.
What To Do:
Puncture Wounds
 To most effectively relieve pain and attenuate some of the thermolabile protein components of the venom, soak the wound in hot (not scalding) water (approximately 45° C [113° F]) for 30 to 90 minutes or longer for pain control. Have the patient use an unaffected limb as a control to test the water temperature and thereby avoid scalding.
To most effectively relieve pain and attenuate some of the thermolabile protein components of the venom, soak the wound in hot (not scalding) water (approximately 45° C [113° F]) for 30 to 90 minutes or longer for pain control. Have the patient use an unaffected limb as a control to test the water temperature and thereby avoid scalding.
 During hot water treatment or while waiting for it to be available, infiltrate in or around the wound with 0.5% bupivacaine or 1% or 2% lidocaine without epinephrine to provide further pain control. When necessary, be generous and add narcotic analgesics.
During hot water treatment or while waiting for it to be available, infiltrate in or around the wound with 0.5% bupivacaine or 1% or 2% lidocaine without epinephrine to provide further pain control. When necessary, be generous and add narcotic analgesics.
 Irrigate larger wounds as soon as possible with a jet lavage of normal saline or dilute 1% povidone-iodine solution (add 10% Betadine to 0.9% NaCl in a 1:10 ratio), and remove visible pieces of spine or debris.
Irrigate larger wounds as soon as possible with a jet lavage of normal saline or dilute 1% povidone-iodine solution (add 10% Betadine to 0.9% NaCl in a 1:10 ratio), and remove visible pieces of spine or debris.
 Obtain radiographs to detect any hidden radiopaque fragments of retained stingray, catfish, or sea urchin spines. Ultrasonography may also be used to locate any remaining pieces.
Obtain radiographs to detect any hidden radiopaque fragments of retained stingray, catfish, or sea urchin spines. Ultrasonography may also be used to locate any remaining pieces.
 When anesthesia is complete and pain has been controlled, thoroughly explore, débride, and irrigate open wounds.
When anesthesia is complete and pain has been controlled, thoroughly explore, débride, and irrigate open wounds.
 Remove fragile sea urchin spines using the same technique as for a superficial sliver (see Chapter 153). Care should be taken in removal of these spines, because they are brittle and may crumble in the wounds. Thin retained spines without symptoms generally are absorbed or extruded; therefore, if difficult or impractical to remove, they can be left in place. Every effort should be made to remove spines adjacent to a tendon or joint. If left in place, treatment should include a 7- to 14-day course of nonsteroidal anti-inflammatories (NSAIDs) (if not contraindicated), and, if a severe secondary reaction occurs, prednisone should be prescribed (unless infection is suspected).
Remove fragile sea urchin spines using the same technique as for a superficial sliver (see Chapter 153). Care should be taken in removal of these spines, because they are brittle and may crumble in the wounds. Thin retained spines without symptoms generally are absorbed or extruded; therefore, if difficult or impractical to remove, they can be left in place. Every effort should be made to remove spines adjacent to a tendon or joint. If left in place, treatment should include a 7- to 14-day course of nonsteroidal anti-inflammatories (NSAIDs) (if not contraindicated), and, if a severe secondary reaction occurs, prednisone should be prescribed (unless infection is suspected).
 Lightly pack larger wounds open for delayed primary closure (see Chapter 143).
Lightly pack larger wounds open for delayed primary closure (see Chapter 143).
 Ensure current tetanus prophylaxis (see Appendix H).
Ensure current tetanus prophylaxis (see Appendix H).
 Prophylactic antibiotics are not required for minor abrasions, superficial punctures, and superficial lacerations. Injuries with potential for serious infection include large lacerations, deep puncture wounds (particularly near joints), and wounds with retained foreign material.
Prophylactic antibiotics are not required for minor abrasions, superficial punctures, and superficial lacerations. Injuries with potential for serious infection include large lacerations, deep puncture wounds (particularly near joints), and wounds with retained foreign material.
 These infection-prone wounds, and any wound in an immunocompromised individual of any type, require antibiotic treatment. Ciprofloxacin (Cipro), 500 mg bid, or doxycycline (Vibramycin), 100 mg bid for adults, and trimethoprim-sulfamethoxazole (Bactrim/Septra), 8 to 12 mg TMP/kg/day divided bid for children, all prescribed for 3 to 5 days, are the most appropriate regimens for coverage of pathogenic marine microbes. The genus Vibrio is particularly common in the ocean and poses a serious risk for immunosuppressed patients. Rapidly progressive cellulitis or myositis indicates Vibrio parahaemolyticus or Vibrio vulnificus. Also known to inoculate marine wounds are Erysipelothrix rhusiopathiae and Mycobacterium marinarum. In the more severe wounds, the recommended initial parenteral antibiotics include cefoperazone (Cefobid), ceftazidime (Fortaz), gentamicin (Garamycin), ciprofloxacin, ceftriaxone (Rocephin), and cefuroxime (Zinacef).
These infection-prone wounds, and any wound in an immunocompromised individual of any type, require antibiotic treatment. Ciprofloxacin (Cipro), 500 mg bid, or doxycycline (Vibramycin), 100 mg bid for adults, and trimethoprim-sulfamethoxazole (Bactrim/Septra), 8 to 12 mg TMP/kg/day divided bid for children, all prescribed for 3 to 5 days, are the most appropriate regimens for coverage of pathogenic marine microbes. The genus Vibrio is particularly common in the ocean and poses a serious risk for immunosuppressed patients. Rapidly progressive cellulitis or myositis indicates Vibrio parahaemolyticus or Vibrio vulnificus. Also known to inoculate marine wounds are Erysipelothrix rhusiopathiae and Mycobacterium marinarum. In the more severe wounds, the recommended initial parenteral antibiotics include cefoperazone (Cefobid), ceftazidime (Fortaz), gentamicin (Garamycin), ciprofloxacin, ceftriaxone (Rocephin), and cefuroxime (Zinacef).
 For infected wounds, obtain both aerobic and anaerobic cultures, and alert the clinical microbiology laboratory that standard antimicrobial susceptibility testing media may need to be supplemented with NaCl to permit growth of marine bacteria. Institute the above-mentioned antibiotics, except for minor wound infections with the classic appearance of erysipelas, which can be treated with erythromycin or cephalexin. Prescribe antibiotics for 7 to 14 days. Hospitalization may be required for severe infections and in those individuals who are immunosuppressed.
For infected wounds, obtain both aerobic and anaerobic cultures, and alert the clinical microbiology laboratory that standard antimicrobial susceptibility testing media may need to be supplemented with NaCl to permit growth of marine bacteria. Institute the above-mentioned antibiotics, except for minor wound infections with the classic appearance of erysipelas, which can be treated with erythromycin or cephalexin. Prescribe antibiotics for 7 to 14 days. Hospitalization may be required for severe infections and in those individuals who are immunosuppressed.
 Provide pain control with NSAIDs and narcotic analgesics as required.
Provide pain control with NSAIDs and narcotic analgesics as required.
 Follow up all wounds in 1 to 2 days with periodic revisits until healing is complete.
Follow up all wounds in 1 to 2 days with periodic revisits until healing is complete.
Focal Rashes
 For fire coral, jellyfish, hydroid, or sea anemone stings, decontaminate the area with a liberal soaking of 5% acetic acid (vinegar). Less effective alternatives include baking soda or a solution of a dilute (¼ strength) household ammonia. Vinegar and ammonia may be applied continuously by applying soaked compresses until the pain is relieved or for 30 minutes.
For fire coral, jellyfish, hydroid, or sea anemone stings, decontaminate the area with a liberal soaking of 5% acetic acid (vinegar). Less effective alternatives include baking soda or a solution of a dilute (¼ strength) household ammonia. Vinegar and ammonia may be applied continuously by applying soaked compresses until the pain is relieved or for 30 minutes.
 The most effective way to control pain is by using hot water (45° C [113° F]) immersion to inactivate the heat-labile protein toxins. Application of vinegar will stabilize any undischarged stinger cells (nematocysts) and prevent further injury.
The most effective way to control pain is by using hot water (45° C [113° F]) immersion to inactivate the heat-labile protein toxins. Application of vinegar will stabilize any undischarged stinger cells (nematocysts) and prevent further injury.
 Any lacerations from fire coral must be anesthetized, explored, and cleansed. Any retained foreign debris must be removed; then the wound should be lightly packed with moist, fine-mesh gauze for delayed primary closure in 3 to 5 days.
Any lacerations from fire coral must be anesthetized, explored, and cleansed. Any retained foreign debris must be removed; then the wound should be lightly packed with moist, fine-mesh gauze for delayed primary closure in 3 to 5 days.
 After decontamination with vinegar, remove any visible large jellyfish tentacles with forceps or double-gloved hands. Remove small particles by applying shaving foam, or some equivalent, and gently shaving the area with a safety razor, dull knife, tongue blade, or plastic card; then clean with an antibacterial soap and flush with water or saline solution.
After decontamination with vinegar, remove any visible large jellyfish tentacles with forceps or double-gloved hands. Remove small particles by applying shaving foam, or some equivalent, and gently shaving the area with a safety razor, dull knife, tongue blade, or plastic card; then clean with an antibacterial soap and flush with water or saline solution.
 Treat any generalized allergic or systemic reactions with antihistamines, corticosteroids, epinephrine, and IV fluids as indicated.
Treat any generalized allergic or systemic reactions with antihistamines, corticosteroids, epinephrine, and IV fluids as indicated.
 When irritation from sponges, bristle worms, or other marine creatures causes erythematous or urticarial eruptions, it usually means that tiny spicules and spinules are embedded in the skin. Apply vinegar compresses to help neutralize toxins and relieve pain. Dry the skin, apply the sticky side of a piece of adhesive tape to the affected area, and peel the tape back to remove these particles. Cosmetic deep-cleansing strips for skin pores (Bioré Pore Perfect) can also be effective if available. Gauze soaked with glue, applied to the area and allowed to dry, is another method of removing embedded particles when the gauze is peeled away.
When irritation from sponges, bristle worms, or other marine creatures causes erythematous or urticarial eruptions, it usually means that tiny spicules and spinules are embedded in the skin. Apply vinegar compresses to help neutralize toxins and relieve pain. Dry the skin, apply the sticky side of a piece of adhesive tape to the affected area, and peel the tape back to remove these particles. Cosmetic deep-cleansing strips for skin pores (Bioré Pore Perfect) can also be effective if available. Gauze soaked with glue, applied to the area and allowed to dry, is another method of removing embedded particles when the gauze is peeled away.
 Residual inflammation can be treated with topical corticosteroids, such as triamcinolone (Aristocort A) 0.1% or 0.5% cream or desoximetasone (Topicort) emollient cream or ointment 0.25% (dispense 15 g and apply tid to qid). A topical steroid in combination with a topical anesthetic can be additionally soothing (e.g., Pramosone cream, lotion, or ointment 2.5% tid to qid). Systemic antihistamines will also be helpful for pruritus, and, on occasion, systemic corticosteroids will be required.
Residual inflammation can be treated with topical corticosteroids, such as triamcinolone (Aristocort A) 0.1% or 0.5% cream or desoximetasone (Topicort) emollient cream or ointment 0.25% (dispense 15 g and apply tid to qid). A topical steroid in combination with a topical anesthetic can be additionally soothing (e.g., Pramosone cream, lotion, or ointment 2.5% tid to qid). Systemic antihistamines will also be helpful for pruritus, and, on occasion, systemic corticosteroids will be required.
 Tetanus prophylaxis should be administered if indicated.
Tetanus prophylaxis should be administered if indicated.
 Provide pain control with NSAIDs and narcotic analgesics as required.
Provide pain control with NSAIDs and narcotic analgesics as required.
 Advise the patient about sun avoidance and the use of sun blocks to prevent possible postinflammatory hyperpigmentation. Hydroquinone (Eldoquin-Forte) 4% skin bleaching cream can be prescribed to be rubbed in bid when hyperpigmentation occurs.
Advise the patient about sun avoidance and the use of sun blocks to prevent possible postinflammatory hyperpigmentation. Hydroquinone (Eldoquin-Forte) 4% skin bleaching cream can be prescribed to be rubbed in bid when hyperpigmentation occurs.
 Check wounds for infection in 2 and 7 days.
Check wounds for infection in 2 and 7 days.
What Not To Do:
 Do not use fresh water or isopropyl (rubbing) alcohol to decontaminate jellyfish stings. It may cause any remaining nematocysts to rupture and trigger additional stinging.
Do not use fresh water or isopropyl (rubbing) alcohol to decontaminate jellyfish stings. It may cause any remaining nematocysts to rupture and trigger additional stinging.
 Do not use full-strength ammonia as a substitute for vinegar compresses. It is a powerful skin irritant.
Do not use full-strength ammonia as a substitute for vinegar compresses. It is a powerful skin irritant.
 Do not constrict limbs tightly.
Do not constrict limbs tightly.
Discussion
Many marine animals have developed systems for attack and defense that on accidental exposure to humans result in envenomation. Most envenomations are not life threatening, often presenting only as minor contact dermatitis or a small puncture wound. Venomous marine organisms can be difficult to identify or may not be seen at the time of envenomation.
Marine animals responsible for envenomation can be broken into two large groups—vertebrates and invertebrates. Venomous vertebrate marine animals include stingrays, lionfish, scorpion fish, stonefish, and catfish, whereas venomous invertebrates include jellyfish, anemones, and fire coral.
Treatment can be based on the nature and appearance of the wound when the specific sea creature cannot be identified.
Although one should always be wary of the possibility for anaphylaxis and cardiopulmonary collapse, particularly in elderly victims with previous sensitization to venom antigens, these complications are rarely seen with stings from creatures found in North American waters.
Stingray victims are generally innocent beach walkers who step on the back of the ray, which reflexively strikes upward with its tail, inflicting a penetrating wound along the upper foot, ankle, or lower leg. Injuries also are sustained to the hand or arm in the process of trying to remove a stingray that has been caught while fishing. The anatomic structure of the stingray’s spine causes a deep, jagged painful wound that may contain fragments of the barb. This barb is located on the dorsum of the proximal portion of the tail. Submersion of the affected area in hot water (43° to 46° C) may help mitigate the pain: in one retrospective review, 65 (67%) of 97 patients with stingray wounds had complete analgesia with hot water immersion alone. Other remedies, including applying the cut half of an onion (Australian), or urinating on the wound are unproven.
Scorpion fish, lionfish, and stonefish stings occur in divers and fisherman, and sometimes in keepers of marine aquariums or those involved in illegal tropical fish trade. (Intravenous stonefish antivenin is indicated in cases of severe systemic reactions to stonefish.) Catfish stings are common when the fish are handled or kicked. Certain catfish species produce venom in glands at the base of the dorsal spine, but most do not, and catfish venom causes only mild local pain, redness, and swelling. Of more concern is the wound caused by the spine and the likelihood of infection that may take months to resolve.
Sea urchin victims are stung when they step on, handle, or brush up against these sessile creatures. The sea urchin secretes a toxin on the surface of its spines that is transferred into the wound when they penetrate the skin. The brittle spines also tend to break off and remain in the wound.
Jellyfish, sea anemones, and fire coral envenomate their prey through nematocysts (Figures 145-3 and 145-4). Nematocysts are venom-containing stinging organelles located in specialized epithelial cells called cnidocytes. Jellyfish tentacles vary in length from a few millimeters to more than 40 meters. Tentacles that have separated from the jellyfish are still capable of stinging for weeks or months after becoming detached, even if dried.
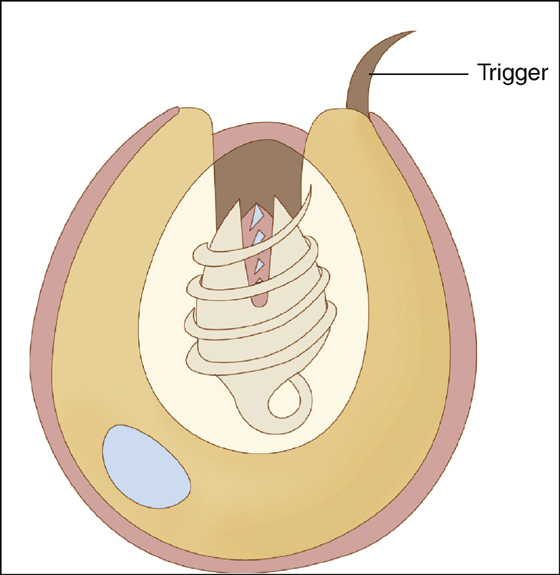
Figure 145-3 Nematocyst prior to discharging. (Adapted from Stauffer AR, Auerbach PS: Marine envenomations: common Florida injuries. EMpulse 8:12, 2003.)
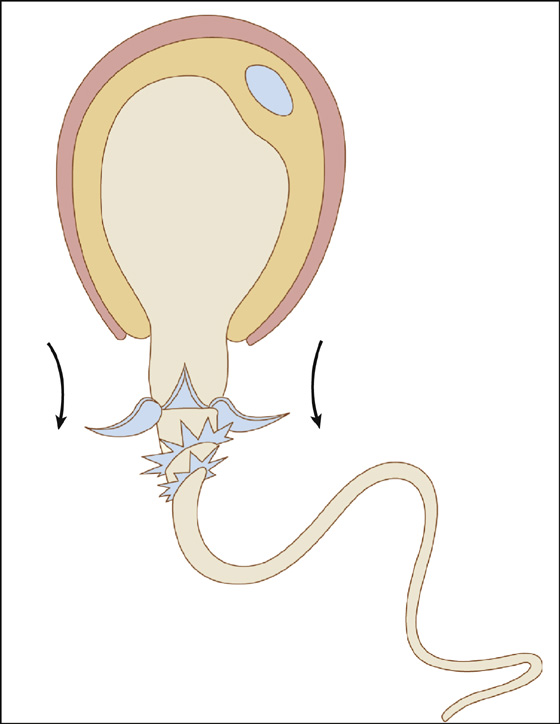
Figure 145-4 Nematocyst after discharge occurs. (Adapted from Stauffer AR, Auerbach PS: Marine envenomations: common Florida injuries. EMpulse 8:12, 2003.)
Although not as effective as heat or vinegar, papain (unseasoned meat tenderizer or papaya latex [juice]) also have been reported to relieve the pain associated with jellyfish stings. If either is used, it should be applied for no longer than 15 minutes. Isopropyl alcohol (which some suggest may worsen the pain), dilute ammonium hydroxide, sodium bicarbonate, olive oil, urine, and sugar are also described in marine medical literature as potentially effective.
“Safe Sea” sunscreen with jellyfish sting protective lotion (Nidaria Technology, Boca Raton, Fla.) is a commercial product that shows promise as an effective “sting inhibitor” when applied to human skin before jellyfish tentacle contact. This product has been studied in two trials involving human volunteers and has demonstrated a clinically important benefit.
The sea wasp, or box jellyfish, which inhabits the Indo-Pacific Ocean, is the most venomous sea creature and can induce death in 30 seconds. If a patient who is stung by this member of the Scyphozoa survives long enough to receive medical care, sheep antivenom is available.
True and soft corals can cause lacerations secondary to mechanical trauma. There is no envenomation, but wounds often become infected, having poor healing and a persistent exudate. These wounds should be carefully cleaned and débrided and treated with daily wet-to-dry dressings until clean.
Minor bites from octopi, sharks, moray eels, and barracudas are usually the result of the marine creature’s instinct to protect itself against a perceived danger. Treatment is symptomatic; local cleansing and topical dressing usually are adequate. If the wound becomes infected, antibiotics as previously described should be initiated.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


