Management of Rosacea and Other Acneiform Dermatoses
Peter C. Schalock
Arthur J. Sober
Rosacea and periorificial dermatitis produce acneiform lesions. Rosacea is particularly common, affecting between 1.5% and 10% of the population, depending on the sample. It most commonly occurs between the ages of 30 and 50 years, although it can be present in individuals both older and younger. Periorificial dermatitis typically presents in women aged 20 to 40 years. The primary care physician should be able to identify these acneiform conditions, differentiate them from other diseases, and institute proper treatment.
Rosacea
Pathophysiology
Rosacea is a chronic inflammatory condition of unknown etiology. Although individuals of all ethnic backgrounds can develop rosacea, it primarily affects patients of Irish, Scottish, Scandinavian, and English descent. The earliest pathophysiologic change is vascular instability, with flushing attributable to a heat-regulating reflex involving the countercurrent thermal exchange between the common carotid artery and the internal jugular vein; substance P and vasoactive peptides may also play a role. Recent linkages to increased amount and activity of cathelicidin and kallikrein 5 have also been suggested. Ultraviolet damage with microscopic evidence of dermal elastotic degeneration is noted in most patients. Demodex folliculorum and Demodex brevis mites have been found at higher concentrations in patients with rosacea, especially those with topical steroid-induced rosacea. Helicobacter pylori infection may contribute to rosacea, possibly through the release of vasoactive substances such as gastrin. Studies on H. pylori have prompted consideration of an association between rosacea and gastritis. A statistically significant incidence of migraine headaches accompanying rosacea has been reported, perhaps indicating a background of vascular reactivity.
Clinical Presentation
Patients exhibit a spectrum of lesions involving the central face, the mildest being erythema producing a red face or ruddy cheeks and flushing in response to hot liquids, spicy foods, alcohol consumption, sun exposure, wind, vasodilating drugs, or emotional factors. Additional lesions include papules and pustules, but not comedones; the latter are specific for acne vulgaris. Telangiectasias may develop as a response to recurrent erythema and flushing, and facial edema may ensue from long-standing erythema. Figure 186-1 shows a case of moderate rosacea. In severe rosacea, rhinophyma, a thick, lobulated overgrowth of connective tissue and sebaceous glands of the nose, may be a feature (Fig. 186-2). Ocular complications commonly include blepharitis, conjunctivitis, episcleritis, and, infrequently, iritis and keratitis.
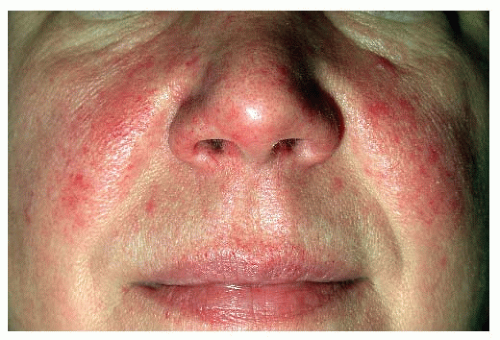 Figure 186-1 Papulopustular and telangiectatic rosacea. (Photo courtesy Peter C. Schalock.) |
Periorificial Dermatitis
Patients present with an erythematous, scaling, papular, or papulopustular eruption around the mouth, chin, upper lip, eyes, and nasolabial folds. The lesions are usually bilateral and symmetric. Occasionally, papulopustular lesions are widespread. Many patients report a stinging sensation associated with these lesions. The course is typically relapsing and remitting, similar to that of rosacea.
The cause of periorificial dermatitis is unknown. Light sensitivity, rosacea, atopy, Demodex mite infestation, candidiasis, overgrowth of the yeast Pityrosporum ovale, and the use of fluoride toothpaste have been implicated. Some cases of perioral dermatitis have been reported as a reaction to dental resins. Controversy exists as to whether use of cosmetics and/or self-manipulation contribute to this disease. The condition can be replicated by chronic use of fluorinated corticosteroid medications.
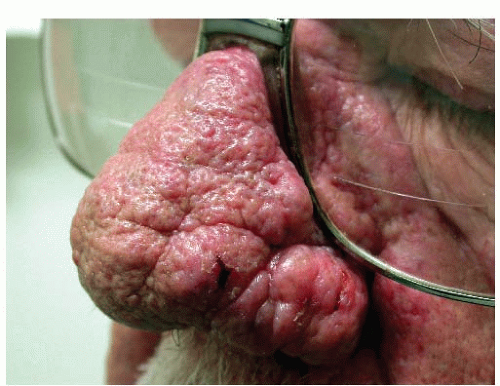 Figure 186-2 Severe rhinophyma in an elderly man. (Photo courtesy Peter C. Schalock.) |
DIAGNOSIS
Rosacea
The diagnosis is made clinically, taking care to differentiate rosacea from acne and other erythematous skin diseases such as seborrheic dermatitis, Pityrosporum folliculitis, contact dermatitis, eczema, and drug-induced photosensitivity. Acne presents in a younger age group and features comedones in addition to papules and pustules. Perioral dermatitis can look like rosacea, and some consider it to be a variant of rosacea. Serious systemic diseases can present similarly to rosacea, including lupus erythematosus and sarcoidosis.
Related posts:
 Screening for HIV Infection
Screening for HIV Infection
 Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


