Prehypertension: Systolic blood pressure (SBP) 120 to 139 mm Hg and diastolic blood pressure (DBP) 80 to 89 mm Hg
Stage 1 hypertension: SBP 140 to 159 mm Hg and DBP 90 to 99 mm Hg
Stage 2 hypertension: SBP 160 mm Hg or greater and DBP 100 mm Hg or greater
of treatment. The task requires determining the degree of blood pressure elevation and identifying other cardiovascular risk factors (e.g., smoking, diabetes, hypercholesterolemia, age, gender, and family history), as well as any manifestations of target organ disease (e.g., left ventricular hypertrophy [LVH] with remodeling, retinopathy, nephrosclerosis, congestive heart failure [CHF], coronary artery disease, stroke, and peripheral vascular disease [see Chapter 19]). For any level of blood pressure elevation, the presence of such features dramatically raises the coronary disease risk from hypertension (e.g., from 9% over 10 years for a 40-year-old man with stage 1 hypertension to 70% for the same 40-year-old man if he also has elevated total cholesterol, a low high-density lipoprotein [HDL] cholesterol, diabetes, and LVH and smokes [see Appendix 26-1-26-26]). Because the risk of hypertension varies significantly depending on what other risk factors are present, the JNC has in the past emphasized an algorithm to guide treatment decisions based on assessment of total cardiovascular risk. In JNC 8, the goals of therapy have been relaxed a bit for high-risk groups due to lack of evidence of benefit from extra-tight control (see Table 26-1).
TABLE 26-1 Management of Hypertension by Blood Pressure Stage and Risk Group | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
to their degree of salt sensitivity; African Americans and the elderly, who tend to have low-renin, volume-expanded hypertension, appear to respond particularly well to sodium restriction. Because we lack effective ways of identifying those most likely to respond to sodium restriction, all patients should be instructed in either a no-added-salt diet (4 g sodium/d) or a lowsodium diet (2 g/d), depending on their volume status. Current evidence finds a daily sodium limit of 1.5 g to be optimal (though hard to achieve). Not only may salt restriction alone provide adequate control in some mild cases, but it also can profoundly affect the efficacy of pharmacologic therapy. Patients receiving diuretics who had an unrestricted salt intake showed a blood pressure reduction of 4%, compared with a 15% reduction for those restricting their sodium intake.
treatment. In JNC 8, the blood-pressure threshold for initiation of pharmacologic therapy in the general population 60 years and older has been raised to 150/90 mm Hg on the basis of seminal studies in the elderly.
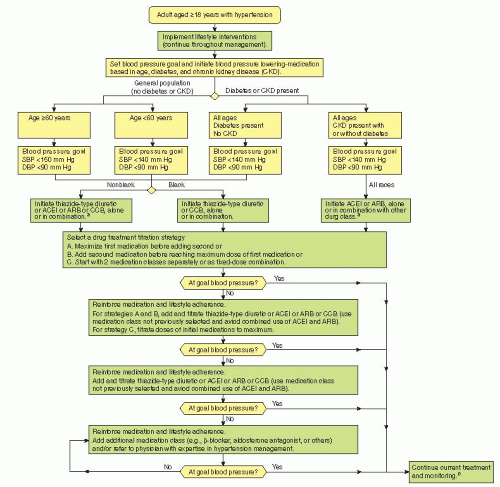 Figure 26-1 2014 Hypertension guideline management algorithm. (SBP, systolic blood pressure; DBP, diastolic blood pressure; ACEI, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CCB, calcium channel blocker. aACEIs and ARBs should not be used in combination. bIf blood pressure fails to be maintained at goal, reenter the algorithm where appropriate based on the current individual therapeutic plan.) (From 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2013;doi:10.1001/jama.2013.284427.) |
weaned off medication with the caveats that they need to continue nonpharmacologic measures and should be monitored periodically because pressures can slowly rise months after stopping therapy.
TABLE 26-2 Lifestyle Modifications for Managing Hypertension | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
TABLE 26-3 Evidence-Based Dosing for Antihypertensive Drugs | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 26-4 Strategies to Dose Antihypertensive Drugs | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
cardiovascular morbidity and mortality. Such proven efficacy, combined with safety and extremely low cost, makes thiazides a compelling first choice for the pharmacologic management of hypertension (Table 26-3). In addition to chlorthalidone, agents included in this class are hydrochlorothiazide (HCTZ) (the most widely prescribed thiazides in the United States), indapamide (commonly used outside the United States), and metolazone.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


