Initial Diagnosis & Management
1. Examine & stabilize—check Airway, Breathing & Circulation
2. Fluid resuscitate—obtain adequate venous access
3. Review data—patient history, anesthesia record, surgical procedure, estimated blood loss, PACU data
4. Consider laboratory studies
• ABG—assess oxygenation & acid–base status
• CBC—assess hemoglobin & platelet level (also consider coagulation studies)
• ECG—assess for arrhythmias (also consider cardiac enzymes)
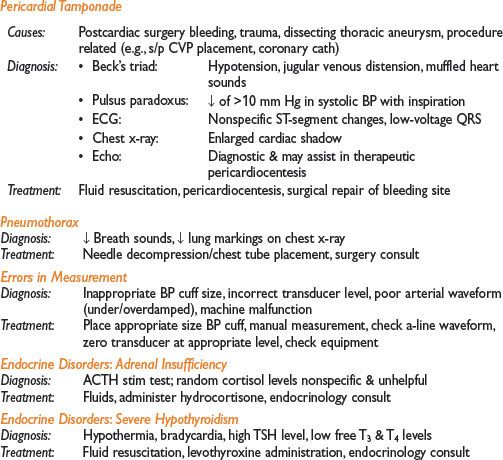
• CXR—rule out pneumothorax/hemothorax/cardiomegaly
• Blood cultures—esp if sepsis suspected
• Transthoracic/transesophageal echo—assess cardiac contractility, LV/RV function, LV filling, IVC collapse, valvular abnl
5. Consider invasive monitoring—arterial BP, CVP, pulmonary artery catheter
6. Initiate pressor/inotropic support—phenylephrine, norepinephrine, dopamine
7. Obtain consultations as needed—cardiology, ICU, surgery
Management of Specific Conditions
Hypovolemia
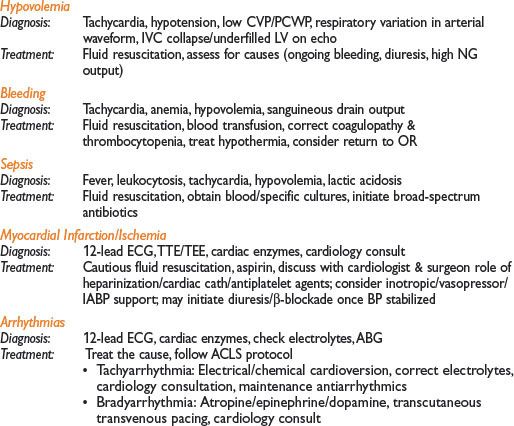
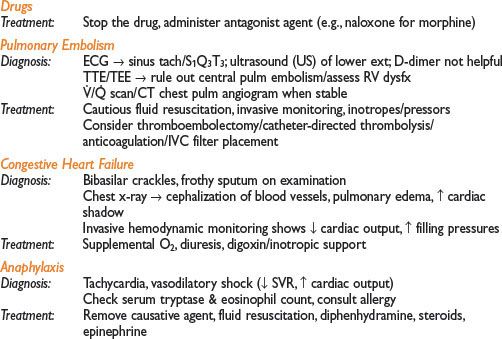
Myocardial Infarction/Ischemia
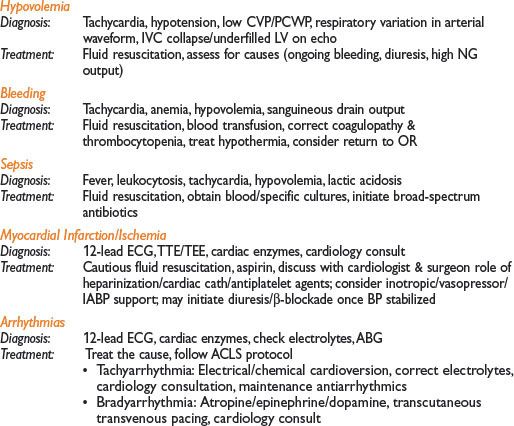
Bleeding
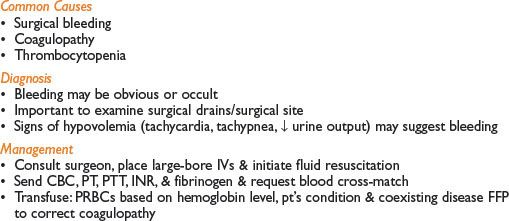
Common Causes
• Cryoprecipitate if evidence of hypofibrinogenemia
• Platelets if level <50,000–100,000 or previous exposure to antiplatelet agents
• Consider use of recombinant factor 7 in uncontrolled, diffuse, postop bleeding
• Assess for evidence of DIC (↓ fibrinogen, + FDP/D-dimer, ↑ PT/PTT, ↓ platelets)
→ Occurs in mismatch transfusion, placental abruption, intrauterine fetal demise, underlying malignancy, complex infections
→ Treat with transfusion of FFP, cryoprecipitate, & platelets
• Maintain normothermia & consider calcium administration during massive transfusion
• Alert OR personnel about need for possible take back
HYPERTENSION
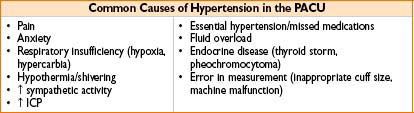
Diagnosis and Management
• Treat the underlying cause
• Resume home antihypertensives as soon as possible
• For initial management consider:
Labetalol 5–40 mg IV bolus q10min or
Hydralazine 2.5–20 mg IV bolus q10–20min or
Lopressor 2.5–10 mg IV bolus
• For severe hypertension, consider vasodilator infusion
Sodium nitroprusside (0.25–10 mcg/kg/min) or
Nitroglycerine (10–100 mcg/min)
Esmolol, nicardipine, cardizem infusions may also be used
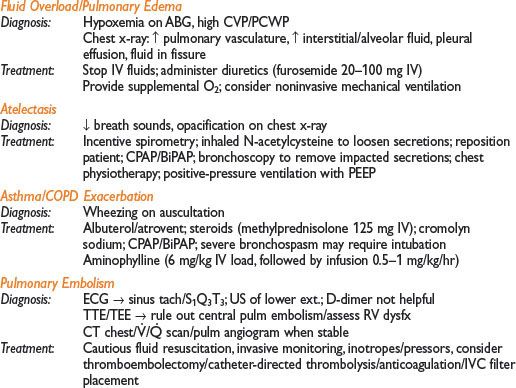
RESPIRATORY AND AIRWAY PROBLEMS
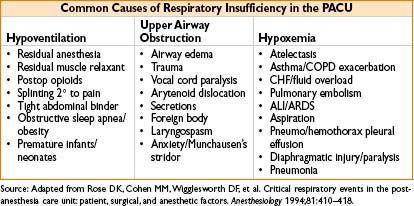
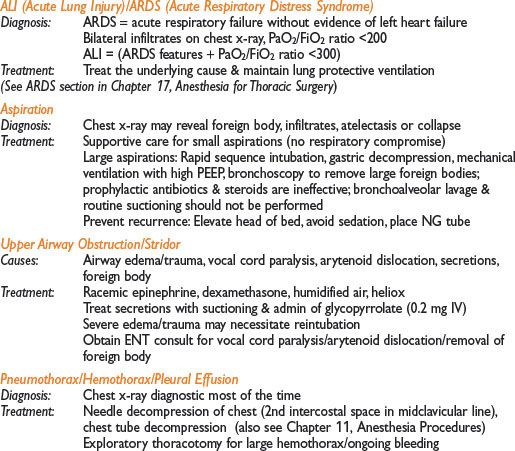
Respiratory Insufficiency: Diagnosis & Management
1. Assess Airway, Breathing, Circulation
2. ↑ delivered FiO2, ↑ flow rate & consider non-rebreather or shovel mask
3. Consider jaw thrust/chin lift, placement of oral/nasal airway
4. Consider positive-pressure ventilation with bag-valve mask
5. Consider intubation vs. noninvasive ventilation (CPAP/BiPAP)
6. Review pt history, OR & postop course, fluid status, & medications administered
7. Consider ABG, chest x-ray (rule out pneumothorax/pulmonary edema)
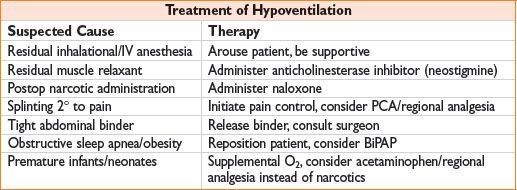
Respiratory Insufficiency: Management of Specific Conditions
Hypoventilation

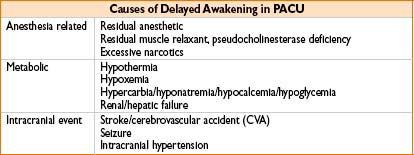
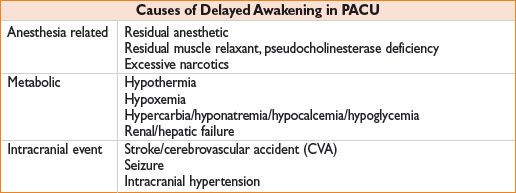
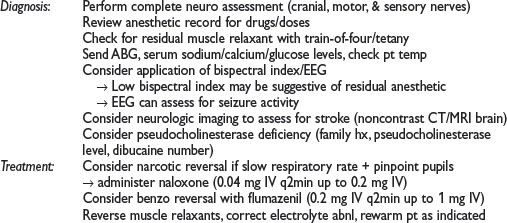
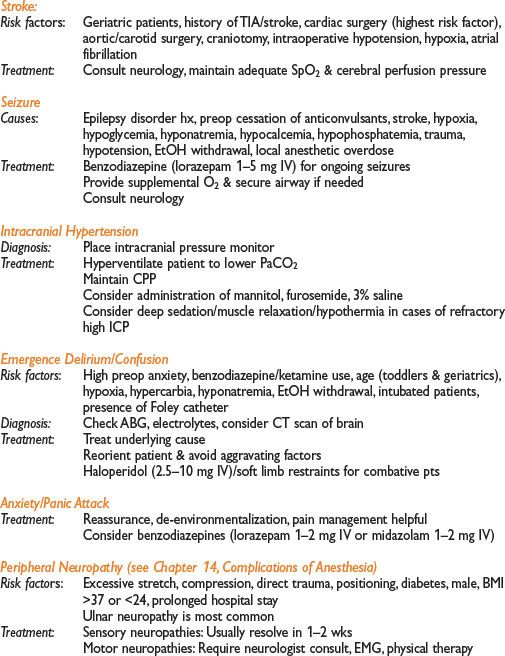
NEUROLOGIC PROBLEMS
Common Problems: Delayed awakening, emergence delirium/confusion, anxiety/panic attack, peripheral neuropathy
Delayed Awakening (see Chapter 10, Common Intraoperative Problems)

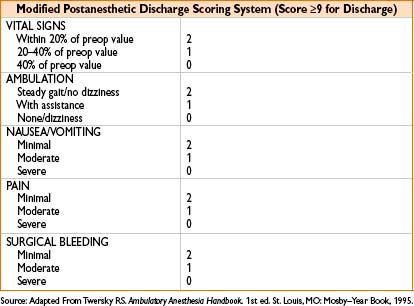
PACU DISCHARGE CRITERIA
• PACU discharge criteria usually based on modified Aldrete score (Anesthesiology 2002;96:742)
• Clinical judgment should always supersede any score or criterion
• Postanesthesia recovery is divided into 2 phases

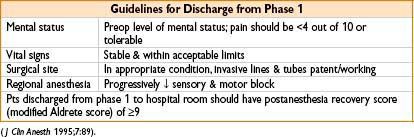
Guidelines for Discharge From Phase 2
• Redocumentation of vitals, postanesthesia recovery score
• Acceptable surgical site condition
• Adequate pain control (<3 out of 10 or tolerable)
• Ability to ambulate
• Recovery from regional anesthesia (except for peripheral nerve block)
• Discharge to a responsible adult
• Postanesthesia recovery score of ≥9
• Written & verbal instructions provided prior to discharge

Common Discharge Issues (Anesthesiology 2002;96:742–752)
• Passing of urine is not a mandatory requirement
• Ability to drink and retain fluids is not mandatory
• There is no minimum PACU stay period
• Escort is needed if pt received any sedation
< div class='tao-gold-member'>









