6 Lumbar Spine and Pelvis ! +++ R2–3 times a week, up to 8 weeks MM, ThE, MET, PhysApps, Chiro ! +++ R 3 times a week, up to 6 weeks MM, MA, ThE, Orthotech
 Complex Pain
Complex Pain
Lumbago
Indications
 Pain conditions in lumbago and coxalgia
Pain conditions in lumbago and coxalgia
 Irritation of the gluteus maximus and the long back extensors
Irritation of the gluteus maximus and the long back extensors
 Affections of the superior iliolumbar ligaments
Affections of the superior iliolumbar ligaments
 Tightening of the paravertebral muscles, as well as pseudoradicular symptoms
Tightening of the paravertebral muscles, as well as pseudoradicular symptoms
Differential Diagnoses
 Blockage of the sacroiliac joint and the L 5 facet
Blockage of the sacroiliac joint and the L 5 facet
 Inflammation of the sacroiliac joint
Inflammation of the sacroiliac joint
 Radicular symptoms in herniated vertebral disks
Radicular symptoms in herniated vertebral disks
 Radiating complaints originating in disorders of the ureter and the bladder
Radiating complaints originating in disorders of the ureter and the bladder
 Referred pain originating in segmental processes (head zone T 11)
Referred pain originating in segmental processes (head zone T 11)
 Tumors in the lower abdomen
Tumors in the lower abdomen
 Instability at the lumbosacral transition
Instability at the lumbosacral transition
Material
 Local anesthetic: 5–10 mL
Local anesthetic: 5–10 mL
 Needle: 0.8 × 80 mm
Needle: 0.8 × 80 mm
Technique
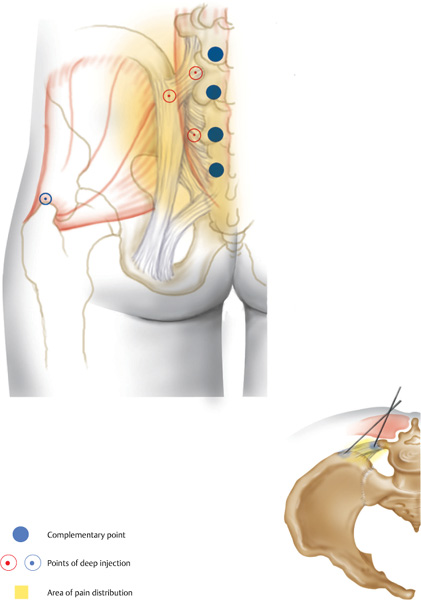
 The superior pelvic crest is palpated 2–3 finger widths paraspinally, at the level of the fifth lumbar vertebral body. The needle is inserted vertically until bone contact is made (transverse process of L 5). A local anesthetic (2 mL) is injected. The needle is then retracted 1–2cm and advanced toward the pelvic crest until bone contact is made. Here, the needle is retracted 2–3 mm and 2–3 mL of a local anesthetic is injected. The needle is inserted again, 2–3 finger widths inferior to the first injection site. The procedure of the first injection is repeated. This results in an almost isosceles triangle being formed.
The superior pelvic crest is palpated 2–3 finger widths paraspinally, at the level of the fifth lumbar vertebral body. The needle is inserted vertically until bone contact is made (transverse process of L 5). A local anesthetic (2 mL) is injected. The needle is then retracted 1–2cm and advanced toward the pelvic crest until bone contact is made. Here, the needle is retracted 2–3 mm and 2–3 mL of a local anesthetic is injected. The needle is inserted again, 2–3 finger widths inferior to the first injection site. The procedure of the first injection is repeated. This results in an almost isosceles triangle being formed.
 Complementary injections may be performed 1finger width paraspinally next to L4/L 5, L 5/S1, and S 1/S 2, comprising a subcutaneous quaddle and an injection close to the bone. Equilateral injection at the greater trochanter is recommended if muscles connecting the pelvis and the greater trochanter are involved.
Complementary injections may be performed 1finger width paraspinally next to L4/L 5, L 5/S1, and S 1/S 2, comprising a subcutaneous quaddle and an injection close to the bone. Equilateral injection at the greater trochanter is recommended if muscles connecting the pelvis and the greater trochanter are involved.
Risks
 Bone contact safeguards unintentional excessive advancement of the needle. If the needle is advanced too far centrally and drops after initial resistance, aspiration has to rule out unintentional administration near the spinal cord (liquor!).
Bone contact safeguards unintentional excessive advancement of the needle. If the needle is advanced too far centrally and drops after initial resistance, aspiration has to rule out unintentional administration near the spinal cord (liquor!).
 Direct infiltration between bone and periosteum should be avoided owing to its extreme painfulness.
Direct infiltration between bone and periosteum should be avoided owing to its extreme painfulness.
Concomitant Therapies
 Dysfunctions of the sacroiliac joint are nearly always present; therefore, mobilization or manipulations of the sacroiliac joint are recommended.
Dysfunctions of the sacroiliac joint are nearly always present; therefore, mobilization or manipulations of the sacroiliac joint are recommended.
 Relaxation techniques and muscular balancing by stretching the quadratus lumborum and muscles connecting the pelvis and the greater trochanter have been proven useful. The patient can repeat the exercises at home.
Relaxation techniques and muscular balancing by stretching the quadratus lumborum and muscles connecting the pelvis and the greater trochanter have been proven useful. The patient can repeat the exercises at home.
 Medical exercise therapy and physical therapy to relax the musculature.
Medical exercise therapy and physical therapy to relax the musculature.
Piriformis Syndrome
Indications
 Frequently, pseudoradicular symptoms in terms of sciatica. Patients complain about pain on the side of the hip when they are lying down at night.
Frequently, pseudoradicular symptoms in terms of sciatica. Patients complain about pain on the side of the hip when they are lying down at night.
 Tendinopathy of the greater trochanter
Tendinopathy of the greater trochanter
 Concomitant treatment of sacroiliac joint dys-functions
Concomitant treatment of sacroiliac joint dys-functions
Differential Diagnoses
 Sciatic irritations
Sciatic irritations
 Affections of the gluteus medius
Affections of the gluteus medius
Material
 Local anesthetic: 5 mL
Local anesthetic: 5 mL
 Needle: 0.8 × 80 mm
Needle: 0.8 × 80 mm
Technique
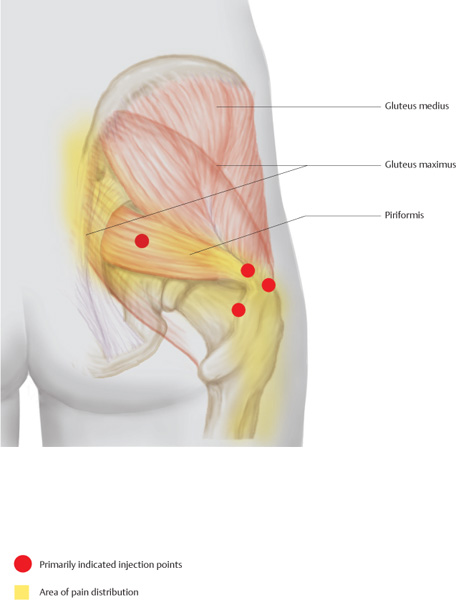
 The greater trochanter is located. At its tip and 2 cm apart, along its posterior edge, the needle is inserted vertically until bone contact is made. After the needle has been retracted 1–2 mm, 1 mL of a local anesthetic is injected at each site.
The greater trochanter is located. At its tip and 2 cm apart, along its posterior edge, the needle is inserted vertically until bone contact is made. After the needle has been retracted 1–2 mm, 1 mL of a local anesthetic is injected at each site.
 At the center, between the greater trochanter and the sacroiliac joint, the trigger point of the piriformis can be found. This is usually a painful area, including a rough palpable myogelosis. The needle is inserted 4 cm and 2 mL of the injectable is administered.
At the center, between the greater trochanter and the sacroiliac joint, the trigger point of the piriformis can be found. This is usually a painful area, including a rough palpable myogelosis. The needle is inserted 4 cm and 2 mL of the injectable is administered.
Risks
 If the needle is advanced excessively, the sciatic nerve may be anesthetized; therefore, the needle must be retracted if radiating, flashlike sensations are reported.
If the needle is advanced excessively, the sciatic nerve may be anesthetized; therefore, the needle must be retracted if radiating, flashlike sensations are reported.
Concomitant Therapies
 Manual therapy in functional disorders of the sacroiliac joint
Manual therapy in functional disorders of the sacroiliac joint
 Physical therapy in terms of stretching of the piriformis, including postisometric relaxation and instructions for self-mobilization. Differences in the length of the legs must be observed!
Physical therapy in terms of stretching of the piriformis, including postisometric relaxation and instructions for self-mobilization. Differences in the length of the legs must be observed!
Periarthritis Coxae
Indications
 Diffuse pain in the hip joint, pain accompanying hip arthrosis
Diffuse pain in the hip joint, pain accompanying hip arthrosis
 Adjuvant treatment in necrosis of the femoral head
Adjuvant treatment in necrosis of the femoral head
 Treatment after placement of a total hip endoprosthesis
Treatment after placement of a total hip endoprosthesis
 Treatment after femoral neck fracture
Treatment after femoral neck fracture
Differential Diagnoses
 Coxitis
Coxitis
 Metastases in older patients
Metastases in older patients
Material
 Local anesthetic: 5 mL
Local anesthetic: 5 mL
 Needle: 0.8 × 80 mm
Needle: 0.8 × 80 mm
Technique
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


