CHAPTER 26 Lumbar Medial Branch Neurotomy
Description
Terminology and Subtypes
Lumbar medial branch neurotomy (LMBN) involves inserting a radiofrequency electrode onto particular lumbar medial branches to deliver an electric current that will coagulate sensory nerves, stop their conduction of nociceptive impulses, and thereby relieve pain thought to originate from the zygapophysial joints. Other terms have been used to describe LMBN, including facet radiofrequency neurotomy, facet rhizotomy, and facet denervation; these terms are incorrect because they refer to a different procedure with a discredited anatomic basis.1,2 The two main types of LMBN are the Dutch technique and the Interventional Spine Intervention Society (ISIS) technique; each is briefly described below.
The term facet joint is an American neologism, coined in the 1970s when surgeons became interested in the small joints of the lumbar spine as a potential source of low back pain (LBP). However, these joints had already been given a formal name which had been in use for centuries and was endorsed by the International Anatomical Nomenclature Committee: zygapophysial joints.3 That term was derived from the Greek words zygos (meaning yoke, connection, or bridge) and physis (meaning growth) because these joints are formed by the small growths that bridge consecutive vertebrae posteriorly.4 A contraction for “zygapophysial joint” that has gained some popularity is “Z-joint.” Although sometimes spelled “zygapophyseal,” the correct spelling is “zygapophysial.”4
History and Frequency of Use
Goldthwaite is sometimes credited for initiating interest in the lumbar Z-joints as a source of pain, but his study actually focused on their role in protecting the L5 vertebra from spondylolisthesis.5 Other physicians and researchers early in the 20th century alluded to these joints indirectly when they attributed LBP to arthritis of the spine.6,7 It was Ghormley who, in 1933, raised the clinical profile of the lumbar Z-joints by introducing oblique view x-rays of the lumbar spine to visualize these structures and observe degenerative changes that may occur as a result of osteoarthritis.8 Interest in the Z-joints faded shortly thereafter when Mixter and Barr proposed that lumbar disc herniations were likely the cause of LBP.9 Others tried to resurrect interest in the lumbar Z-joints during the 1940s, but the concept lay mostly dormant for another 30 years.10
Hirsch and colleagues then reported experiments in which noxious stimulation applied to the lumbar Z-joints produced pain in volunteers, but that work attracted little clinical interest.11 More attention was paid in 1971 when Rees reported a success rate of 99.9% in treating LBP using an operation in which the nerves from the lumbar Z-joints could be transected percutaneously with a special scalpel blade.12,13 Other surgeons attempted to reproduce these results but were unable to do so.14–17 Anatomic studies eventually proved that the Rees procedure could not possibly denervate the Z-joints because their nerves were not located where the scalpel had been inserted.18,19
Nevertheless, Shealy became intrigued by the proposition that LBP arising from the Z-joints could be treated by denervating them, and developed a procedure by which the nerves from these joints could be coagulated percutaneously using a radiofrequency electrode similar to that used to treat trigeminal neuralgia. This procedure was called facet denervation, and several descriptive studies were published and reported generally successful results.20–23 Others successfully adopted the Shealy procedure with equally positive outcomes.24–40 However, subsequent anatomic studies reported that the anatomic basis of this procedure was flawed as there were no sensory nerves where the electrode was placed; this raised serious questions about the validity of the procedure.1,2 These reports did not deter clinicians interested in using this procedure, and reports of its efficacy have continued to emerge even as recently as 1997.41 Even a controlled trial purportedly showed positive results for a procedure with no anatomic basis.42
Notwithstanding the uncertainties about how to treat LBP associated with lumbar Z-joints, Mooney and Robertson demonstrated that these joints could be a source of LBP in normal volunteers and that certain patients could be relieved of their pain by anesthetizing these joints.43 Other important findings in the history of this procedure were that pain from the Z-joints could be referred distally into the lower extremity and accompanied by hamstring tightness that limited straight-leg-raising, mimicking some of the features of sciatica. Findings of LBP being induced by Z-joint stimulation in normal volunteers were reproduced, with subsequent pain relief achieved by anesthetizing the joints.44,45 These studies formed the basis for the concept of “facet syndrome” in LBP, which should more properly be referred to as “zygapophysial joint pain” or “Z-joint pain.”
These developments prompted interest in the clinical diagnosis of lumbar Z-joint pain, the use of injection techniques for its diagnosis, and appropriate means of treatment in selected patients. Some investigators claimed that certain clinical features were indicative of lumbar Z-joint pain while others disagreed, but these studies used only single diagnostic blocks that did not control for false-positive responses.46,47 Other studies using controlled diagnostic blocks reported that no clinical features were pathognomonic for the diagnosis of lumbar Z-joint pain, and that computed tomography (CT) was not able to make this diagnosis.48–50 More recently, a set of decision rules was designed to diagnose lumbar Z-joint pain, but the positive predictive value of the rules was weak and achieved only weak diagnostic confidence.51–53 Subsequent studies refuted these rules, which were also based on single diagnostic blocks.54,55
The failure of multiple studies to identify any clinical features that are indicative of lumbar Z-joint pain leaves LMBBs as the only reliable and valid method of identifying this entity in those with LBP. Although some physicians, particularly interventional radiologists, have advocated that Z-joint intra-articular injections could serve both diagnostic and therapeutic purposes, this procedure has never been tested for its validity as a diagnostic test.56–70 In contrast, controlled diagnostic LMBBs have been validated and now constitute the best available method to identify lumbar Z-joint pain.
Practitioner, Setting, and Availability
LMBBs should only be performed by a trained physician able to interpret the patient’s response in the context of the presenting complaint, history, and current psychosocial circumstances to determine if the patient is an appropriate candidate for LMBN. Physicians performing both LMBBs and LMBN should also be trained to recognize and deal with possible complications promptly. This training requires extensive knowledge of spinal anatomy to correctly guide and interpret the various radiographic views before and during the placement of the needle or electrode, and knowledge of how to adapt to local variations in anatomy to recognize procedural errors before incurring complications. ISIS has prescribed guidelines for how LMBBs and LMBN should be performed and regularly conducts postgraduate courses based on these guidelines.71,72 These procedures can be performed in any facility that has a fluoroscopy suite, which is mandatory for the procedures to be accurate and valid. This limits the availability of LMBN to specialty spine clinics, pain management clinics, or hospitals.
Procedure
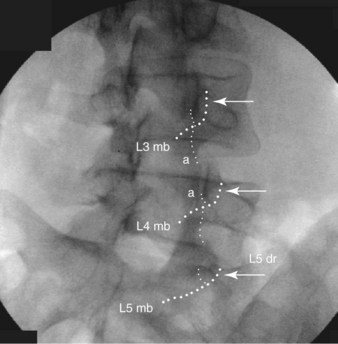
LMBN first requires that diagnostic LMBBs be conducted in order to identify patients with LBP who may benefit from this procedure; blocks are described below. LMBN requires placing a radiofrequency electrode parallel to the target nerve. This involves inserting the electrode from below, so that it crosses the neck of the superior articular process at the target level (Figure 26-1). A thermal lesion is generated by maintaining a temperature of 80° C to 85° C at tip of the electrode for 90 seconds. Depending on the gauge of the electrode used, and the length of its active tip, two or more lesions may need to be placed in various locations to accommodate possible variations in the exact location of the nerve. Details concerning how to place the electrode and perform the procedure accurately and safely are described later in this chapter.71
Dutch Technique
Although the Dutch technique is widely practiced, materials to describe the procedure are unclear. For example, one illustration depicts electrodes placed on the tips of the transverse processes, nowhere near the target nerve (Figure 26-2). Another shows electrodes in positions where lesions would likely fail to incorporate the target nerve fully (Figure 26-3). One version of the Dutch technique that appears anatomically accurate is that of van Kleef and colleagues,75 but in this technique, the electrodes are placed perpendicular to the lumbar medial branches, which lessens the effectiveness of the procedure.
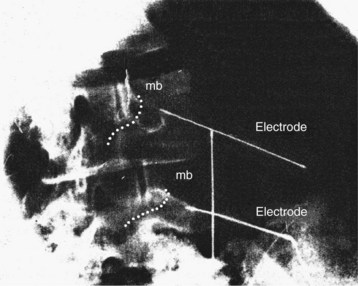
Figure 26-2 A reproduction of an illustration of electrodes in position for lumbar radiofrequency denervation, as depicted by Sluijter and Mehta.73 The electrode position is as depicted in the original. Added are the courses of the medial branches (mb) at the levels targeted.
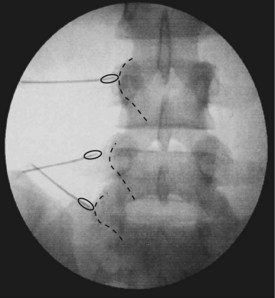
Figure 26-3 A reproduction of a radiograph showing electrodes in position for lumbar radiofrequency denervation, as depicted by van Wijk, et al.74 Added to the illustration are the courses of the lumbar medial branches at the target levels and ellipses that estimate the size and location of the lesions made by the electrodes.
ISIS Technique
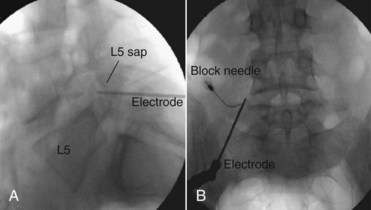
The technique promoted by the ISIS evolved from “facet denervation” through two modifications: (1) the electrodes are placed accurately on the target nerves; and (2) the electrodes are placed parallel to those nerves, rather than perpendicular (Figure 26-4).71 Radiographic anatomy studies have shown that when placed in this manner the electrodes coagulate a substantial length of the target nerves, which correlates with the duration of relief obtained.76
Theory
Mechanism of Action
LMBBs relieve pain through the action of local anesthetic on the sodium channels of the target nerve. The effect is temporary, and relates to the duration of action of the agent used. LMBN exerts a far more lasting effect because the nerve is physically altered. Histologically and physiologically, thermal coagulation at temperatures greater than 80° C affects motor fibers and sensory fibers of all calibers in a nonselective manner.77,78 Coagulation denatures the nerve, and stops conduction of nociceptive traffic, thereby relieving pain. Although the nerve eventually regenerates, the rate of regeneration is slower following LMBN than after traumatic nerve injuries.
When nerves are transected, axon tubules regenerate within hours of the injury, cross the gap, and grow into the distal segment at a rate of 1 mm per day. In contrast, radiofrequency thermal coagulation (as performed in LMBN) seals the nerve in situ, providing no gap across which the nerve can regenerate. Before regeneration can occur into the distal segment, the coagulated segment must be repaired by endocellular processes, which may take several months. Because the time for repair is proportional to the length of segment coagulated, the duration of relief from pain is much longer if a longer length of nerve is coagulated. Because radiofrequency electrodes make small lesions beyond their tip but long lesions along their tip, longer pain relief occurs if electrodes are placed parallel to the nerve than if they are placed perpendicular to the nerve.79
Indication
The clinical indication for LMBBs is unresolved CLBP requiring further investigation, as determined by the physician, patient, and third-party payers (if any). This indication is tempered by the variable prevalence of Z-joint pain. Among injured workers with LBP, its prevalence was 15%, but other studies place the figure at less than 5%.47,48,54,55,80 In older patients without a history of injury, the prevalence is higher, with approximately 30% of patients with LBP reporting at least 90% relief after placebo-controlled LMBBs.81
ISIS guidelines recommend that younger patients are far less likely to respond to LMBBs than older patients, and that physicians first consider discogenic pain or sacroiliac joint pain as an etiology for CLBP.82 Furthermore, the protocol recommends that once LMBBs are initiated, a screening block of all levels liable to be symptomatic first be performed. This is intended promote efficiency and cost effectiveness. The pretest probability is that blocks at all levels will be negative. A single screening block will identify negative patients in one step, and obviates performing repeated blocks at multiple levels only to discover that all are negative. If a screening block is positive, repeat blocks at individual levels can be justified to establish one or more symptomatic joints. For LMBN, the singular indication is complete relief of pain after controlled, diagnostic LMBBs. The ideal patient for LMBBs is one with CLBP worthy of investigation, who has no other sources of pain, is older, and does not have any psychosocial comorbidity. The ideal patient for LMBN is one who tests positive to LMBBs.
Assessment
Before receiving LMBN, patients should first be assessed for LBP using an evidence-based and goal-oriented approach focused on the patient history and neurologic examination, as discussed in Chapter 3. Clinicians should also inquire about medication history to note prior hypersensitivity/allergy or adverse events (AEs) with drugs similar to those being considered, and evaluate contraindications for these types of drugs. Advanced diagnostic imaging such as CT or magnetic resonance imaging is typically required to rule out other potential anatomic causes of CLBP. Interventional diagnostic testing in the form of LMBBs is also required to identify appropriate candidates for this intervention and are described below.
Lumbar Medial Branch Blocks
LMBBs require depositing a small volume of local anesthetic accurately and safely onto each of the two nerves that innervate the target joint. A volume of 0.3 mL is sufficient and larger volumes do not improve the accuracy of the block; excess injectate leaves the vicinity of the target nerve. At typical lumbar levels, the target point lies on the neck of the superior articular process, which the medial branch crosses (see Figure 26-4B). At the L5 level, it is the L5 dorsal ramus, rather than the medial branch, that crosses the neck of the superior articular process of S1; and the dorsal ramus is the target nerve, not its medial branch. Two medial branches innervate each Z-joint but the segmental nomenclature is post-fixed.83,84 For example, the L4-5 Z-joint is innervated by the L3 and L4 medial branches, and the L5-S1 joint by the L4,5 nerves. To avoid confusion in communications and records, ISIS recommends that hyphens between numbers (e.g., L2-3) be used to refer to joints, whereas commas (e.g., L2,3) refer to nerves.85
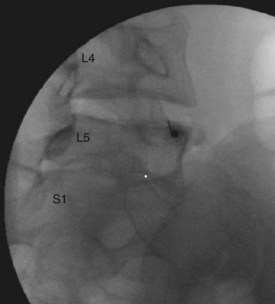
The technique for LMBBs has been described in detail elsewhere.71 Essentially, under fluoroscopic guidance, a needle is introduced directly onto the target point for the nerve (Figure 26-5). Once the needle has been correctly placed, a test dose of contrast medium is injected to test for venous uptake. In the absence of venous uptake, 0.3 mL of local anesthetic agent is injected. The procedure is repeated for each of the nerves that need to be blocked. For blocks to be valid, they must be performed under controlled conditions in each and every patient. Single diagnostic blocks are not valid and carry a false-positive rate of between 25% and 41%.86–89
In the past, comparative local anesthetic blocks have been used to serve as controlled blocks; this involves performing the same block on two separate occasions but using a different local anesthetic agent on each occasion. A positive response is defined as complete relief of pain after each block for the duration of action of the agent used.72,86,87 A recent analysis, however, has shown that comparative local anesthetic blocks are not valid for the diagnosis of lumbar Z-joint pain.90 Comparative blocks have a sensitivity of 100% but a specificity of only 65%.86,90 When the prevalence of lumbar Z-joint pain is low, a specificity of 65% results in a prohibitively high incidence of false-positive responses, far in excess of the prevalence of the condition. Depending on the exact prevalence, for every true-positive response there will be two, three, or more false-positive responses, and the operator cannot tell which is which.90 In effect, operators who rely on comparative blocks will be wrong in their diagnosis far more often than they will be correct.
Placebo-controlled LMBBs are the only means by which to secure confidence in a diagnosis of lumbar Z-joint pain.90 These require blocks on each of three occasions. On the first occasion, a local anesthetic agent is used, in order to establish, prima facie, that the target joint is symptomatic. The second block should use either a local anesthetic agent or a placebo, randomly assigned on a double-blind basis. The third block uses the agent not used for the second block. A positive response is complete relief whenever a local anesthetic is used, and no relief when placebo is used.
ISIS guidelines require that patients be evaluated for a minimum of 2 hours after the block, or until pain relief ceases, whichever occurs first.72 Relief of pain must be recorded in terms of a visual analog scale (VAS) or numerical pain rating scale. Moreover, the relief should be corroborated by the restoration of activities that previously were precluded or limited by pain. Optimally, the physical response should be accompanied by a narrative record of how the patient described and valued the relief.
It has never been shown that patients commonly have multiple sources of pain, and that a 50% relief after LMBB can be a valid sign of lumbar Z-joint pain. Studies have indicated that in patients with CLBP, the prevalence of combined discogenic and Z-joint pain, or sacroiliac joint and Z-joint pain, is less than 5%.91,92 When a pain source can be detected, it is typically one or the other of these structures. Under those conditions, 50% relief of pain is at best a spurious response, and cannot be held as a positive response. The notion of multiple, simultaneous sources of pain can be sustained only if simultaneous anesthetization of the Z-joints and the other source of pain completely relieves the patient’s pain.









