CHAPTER 24
Lumbar Facet Joint Cyst Drainage and Injection
INDICATIONS
The indications for injections of the facet joint include:
• Facet-mediated low back pain
• Diagnostic blocks of facet-mediated low back pain
• Paravertebral spasm
• Facet joint arthritis
• Facet joint effusions
• Facet-mediated pain in rheumatoid arthritis
• Facet-mediated pain in ankylosing spondylitis
• Patients with relief from anesthetic blocks of the facet joint
• Facet joint cysts
Facet joint cysts are associated with facet joint arthropathy, degenerative disc disease, and degenerative spondylolisthesis and cause lower back pain, unilateral radicular pain, neurogenic claudication, and cauda equina syndrome. Most patients with lumbar cysts are in their sixties with a slight female predominance.
RELEVANT ANATOMY
• Each spinal segment is a “three-joint complex” comprised of an interveterbral disc anteriorly and paired posterior synovial facet joints.
• On axial imaging, the facet joints approximate a C or J shape.
• Each joint influences the other two, with degenerative changes in one, affecting the entire complex.
As the intervertebral discs degenerate and the outer annular fibers begin to fragment, the posterior load increases and allows excessive facet joint motion to occur. This abnormal motion accounts for excessive shear forces in the facet joint, resulting in degradation of the cartilage and joint effusion formation. The facet capsule helps limit axial rotation.
• An intact capsule holds 1 to 2 mL of joint fluid with larger effusions implying a loss of capsular integrity and abnormal joint motion (Figure 24-1).
• The facet joint cysts are intraspinal extradural masses, located lateral to the thecal sac and adjacent to the arthritic facet joint ((36)) (Figure 24-2).
• They are most commonly found at the L4-L5 segment, followed by L5-S1, L3-L4, and L2-L3. ((37)).
• The cysts represent synovial exvaginations that arise secondary to recurrent joint effusions and may be considered similar to Baker cysts in the popliteal fossa.
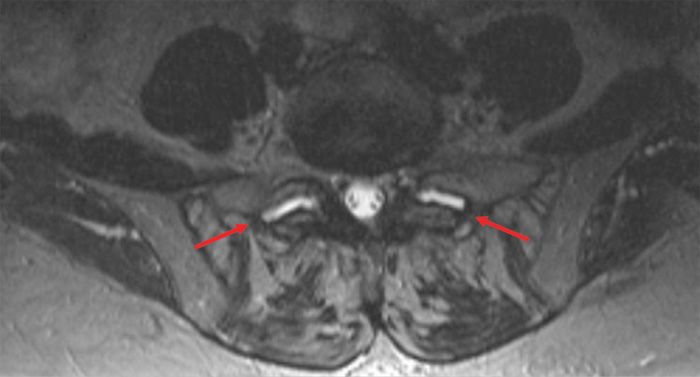
Figure 24-1. Facet effusions.
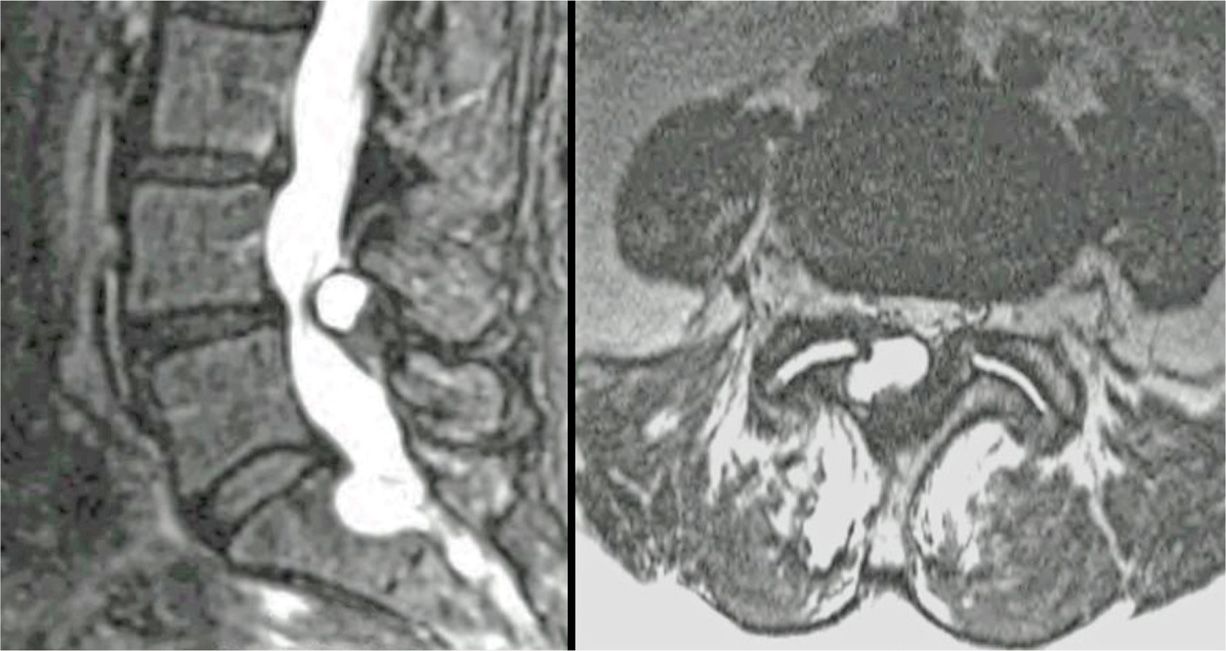
Figure 24-2. Facet joint cysts.
BASIC CONCERNS AND CONSIDERATIONS
The initial radiographic assessment of patients presenting with lumbar facet-mediated pain begins with standard radiographs including AP, lateral, and oblique views. The curved configuration and sagittal orientation of the lumbar facet joint generally limits the utility of frontal and lateral views.
• CT scan more accurately determines the extent of the degenerative changes, but it is poor for evaluation of the presence of facet fluid or cystic formation.
• MRI scanning underestimates the extent of the severity of the osteoarthritic changes, but it is highly sensitive to facet joint fluid and the assessment of the facet cyst.
• The classification of the facet arthropathy by CT scan or MRI can be performed using the Pathria or Fujiwara classifications, respectively.
• Higher grades of facet joint osteoarthritis are more likely to have larger facet joint effusions and synovial cysts.
• The facet joint cysts are usually located anterior and medial to the facet joint.
• The size, location, T2 signal of the facet cyst, and juxtaposition to the neural elements should all be taken into consideration when determining the need for facet cyst drainage and corticosteroid injections.
Facet joint tropism should be noted on axial images. Facet joints are more sagittally oriented in patients with degenerative spondylolisthesis. Facet joint with >45 degrees relative to the coronal plane are 25 times more likely to develop joint effusions and degenerative spondylolisthesis (Figure 24-3). Facet joint effusions associated with facet joint gapping of >1.5 mm are highly predictive of the development of facet joint cysts and degenerative spondylolisthesis.
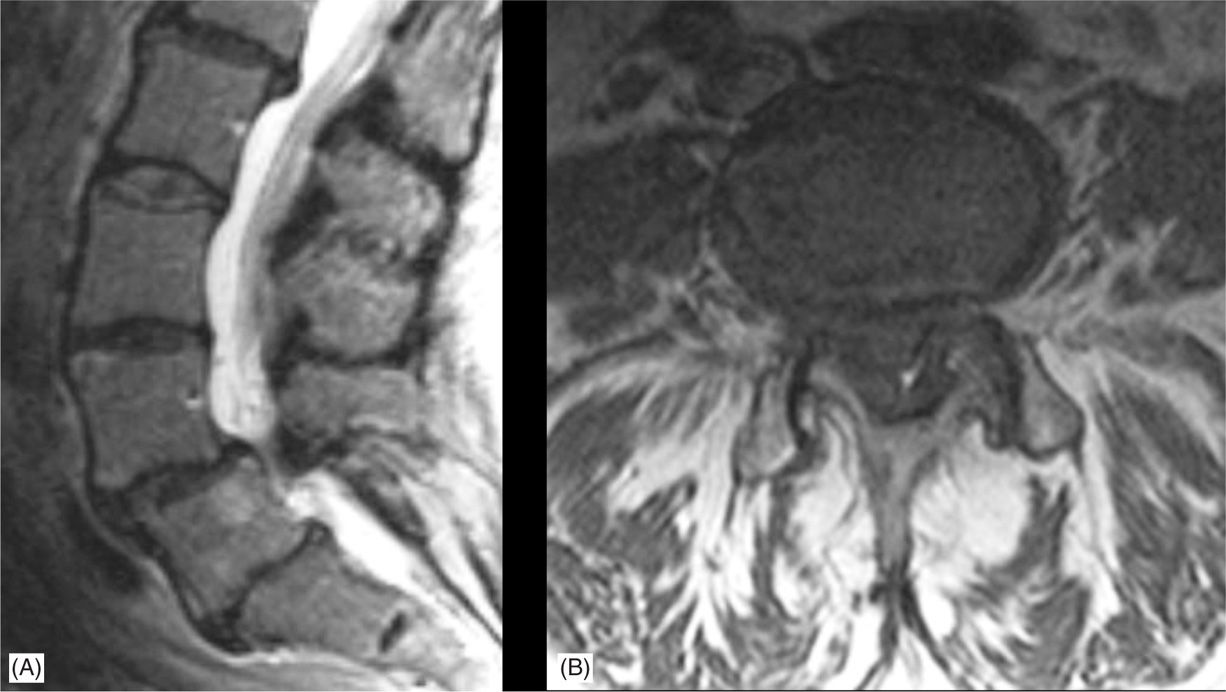
Figure 24-3. Grade 1 L4-L5 spondylolisthesis. (A) Sagittal MRI. (B) Axial MRI.
PREOPERATIVE CONSIDERATIONS
• Informed consent and proper explanation of all risks and complications.
• Anticoagulation. Since the facet joint cyst is extradural and intraspinal, precaution needs to be taken for those on anticoagulants. It is preferable for anticoagulants to be discontinued in adequate time prior to the procedure.
• A baseline musculoskeletal and neurologic physical examination should be performed.
• The patient must be able to lie prone for the duration of the procedure.
• IV access is not necessary for this procedure.
• Evaluate the patient for contrast allergy.
• Septic arthropathy. Lumbar facet joints are uncommon sites of hematologic spread of pyogenic organisms. Must rule out septic arthritis typically unilaterally at L4-L5 facet level (Figure 24-4). These patients present with:
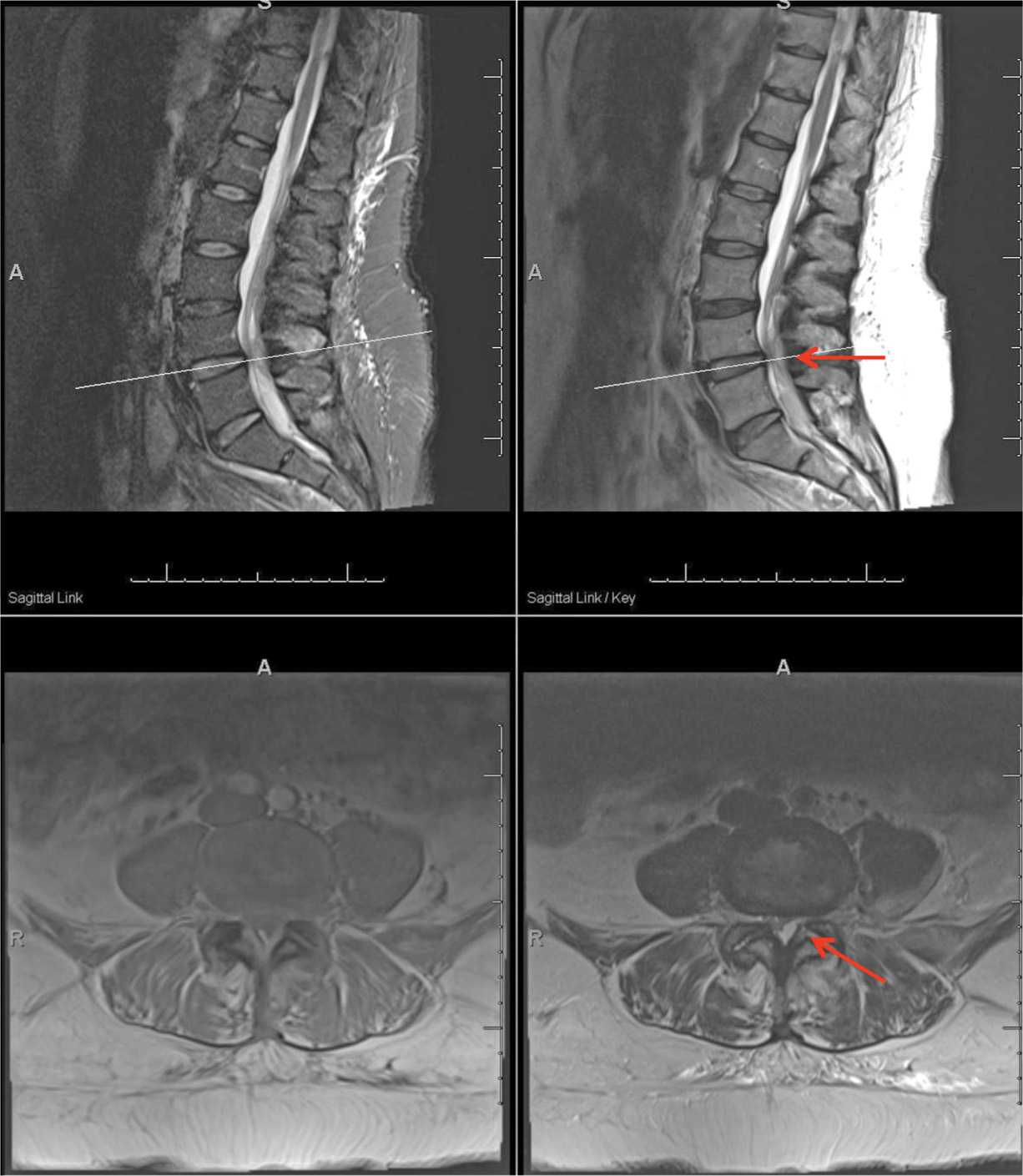
Figure 24-4. Left L4-L5 facet joint septic arthritis with facet cyst and epidural abscess.
![]() Activity associated with stiffness.
Activity associated with stiffness.
![]() Fever and asthenia.
Fever and asthenia.
![]() These symptoms may be present in spondylodiskitis.
These symptoms may be present in spondylodiskitis.
![]() Inflammatory markers including erythrocyte sedimentation rate and C-reactive protein level may be elevated with or without leukocytosis.
Inflammatory markers including erythrocyte sedimentation rate and C-reactive protein level may be elevated with or without leukocytosis.
![]() An MRI with contrast and a radionuclide bone scan would be able to differentiate a facet cyst from a septic arthropathy.
An MRI with contrast and a radionuclide bone scan would be able to differentiate a facet cyst from a septic arthropathy.
Preinjection Pearl
Identification of neurologic impairment associated with the compression of the neural structures associated with the facet joint cyst is the most important preoperative consideration. Motor weakness is not a contraindication for the procedure, although care is needed in pressurization and drainage of the cyst.
Fluoroscopic Views
• Oblique view. The best view for visualization of the facet joint cyst is the oblique view after insertion of contrast medium into the associated facet joint (Figure 24-5).
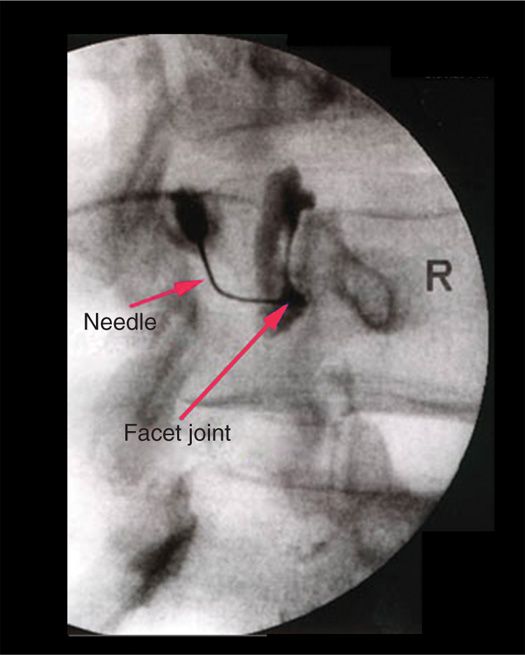
Figure 24-5. Fluoroscopic view of facet joint cyst injection. Note filling of facet cyst.
Equipment
• 25-gauge 0.5-in needle
• 20-gauge 3-in spinal needle
• Syringes: 10, 5, and 3 cc
Medications
• Anesthetic. Preservative-free lidocaine 1%
• Contrast medium. Omnipaque
• Corticosteroid. Depomedrol or Kenalog 40 mg/cc
Technique
There have been reports of a few different procedures to treat facet joint cysts:
• Interlaminar epidural corticosteroid injection under fluoroscopic guidance (extracyst injection)
• Transforaminal epidural corticosteroid injection under fluoroscopic guidance (extracyst injection)
• Cyst drainage by direct puncture (direct method) under CT guidance
• Intra-articular facet joint injection and cyst drainage (indirect method)
The extracystic placement of corticosteroids may temporarily eliminate the radicular component but does not adequately address the cause of the radiculopathy. Direct intracyst injection allows the cyst to reaccumulate fluid as the source of the cyst is excessive production of synovial fluid. The intra-articular injection accomplishes all needs for addressing the pathology. It addresses the pressure of the cystic structure by causing it to leak and treat the joint effusion.
Our Preferred Technique
• The patient is placed prone and prepped.
• The angle of the facet joint is determined by fluoroscopy.
• A lidocaine wheel is made in the skin over the facet joint.
• A 20-gauge 3-in spinal needle is placed through the paraspinal muscles and into the facet joint.
• Placement of the needle bevel entirely in the joint ensures that proper pressurization will take place.
• With the needle bevel in the facet joint, the contrast medium is inserted to confirm placement.
• Once the placement is confirmed, additional contrast material is injected into the joint by maintaining pressure on the syringe.
• The facet joint itself should accept 1 to 2 cc contrast after which the facet cyst fills.
• Syringe pressurization and injection of contrast material continues until there is a loss of pressure indicating a leakage of the cyst and the creation of an epidurogram (Figure 24-6).
• 0.5 to 2 cc of the 1:1 mixture of preservative-free corticosteroid with lidocaine is placed into the joint.
• The needle is withdrawn and sterile band-aid is applied.
• The procedure can be repeated if radicular pain returns.
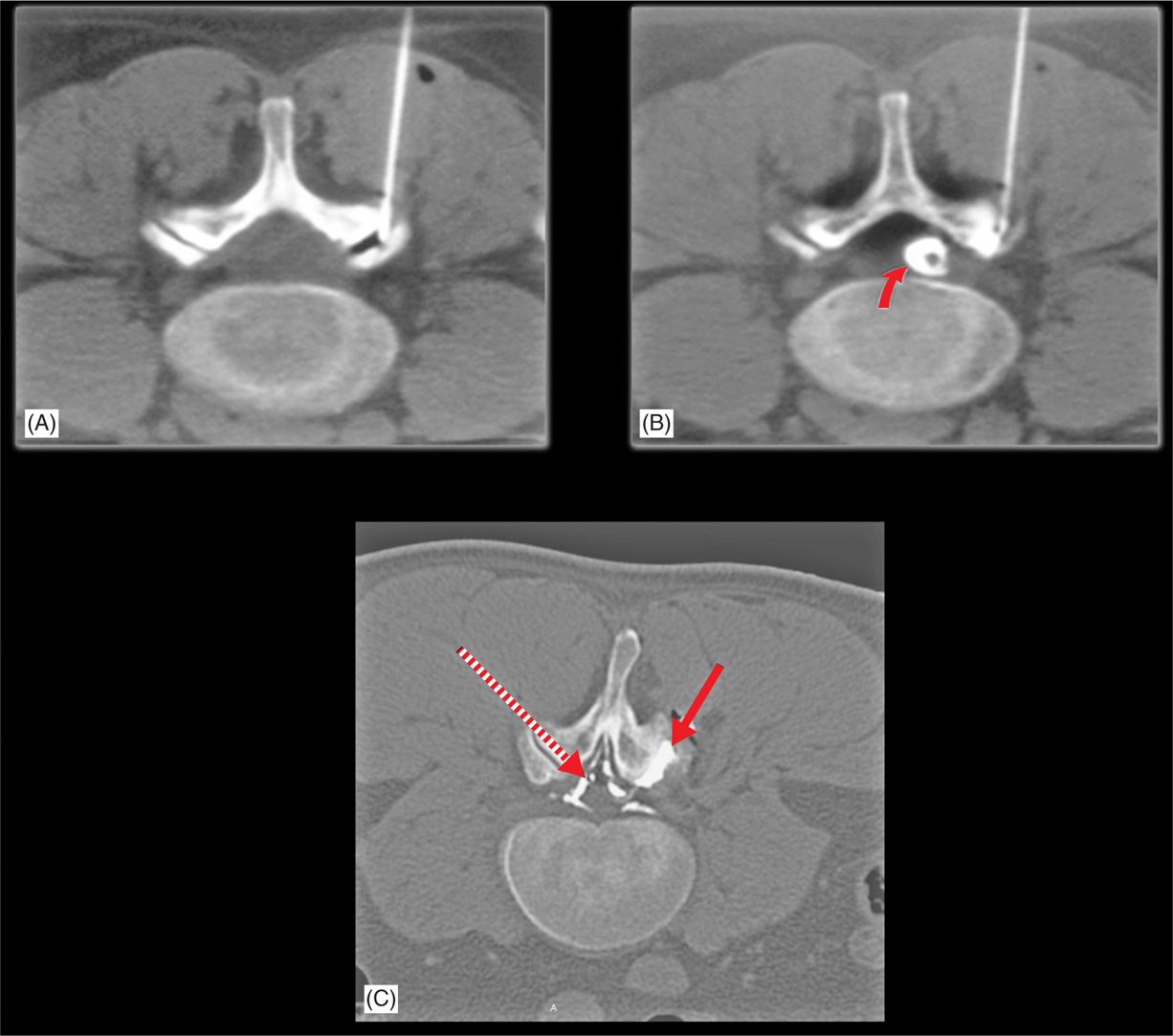
Figure 24-6. Facet injection by CT scan. (A) Needle in facet joint. (B) Needle with contrast into facet joint and cyst filling (curved arrow). (C) Contrast in cyst (solid arrow) and leaking into epidural space (epidurogram) (dotted arrow).
POSTPROCEDURE FOLLOW-UP
Follow-up neurologic assessment is necessary to determine if there is change due to the expansion and subsequent drainage of the facet joint cyst. Follow-up injections are often necessary to continue to reduce the inflammatory response and facet joint effusion.
Potential Complications and Pitfalls
• Incomplete penetration of the facet joint with failure to pressurize the cyst and extravasation of contrast.
• Failure to pressurize the facet cyst will result in incomplete cyst drainage.
• Chronic cysts with thickened capsules or thicker content may not drain well and require repeat injections or failure of the procedure.
CLINICAL PEARLS
• These injections can be very rewarding with complete relief in pain after the initial episode of procedural increase in radicular pain.
• Surgical options would include a laminectomy, cyst excision, and medial facetectomy. If a spondylolisthesis is found on standing or flexion/extension radiographs, fusion may be considered.
Related posts:
 Corticosteroids: Inditoc-authortions, Pharmacology, and Risks in Interventional Pain Management
Corticosteroids: Inditoc-authortions, Pharmacology, and Risks in Interventional Pain Management
 Surgical Treatment of Trigeminal Neuralgia
Surgical Treatment of Trigeminal Neuralgia
 Viscosupplements and Steroid Injections
Viscosupplements and Steroid Injections
 Sacroiliac Joint Denervation by Using Simplicity III
Sacroiliac Joint Denervation by Using Simplicity III
 Commercially Available Reservoir Options for Intrathecal Drug Delivery
Commercially Available Reservoir Options for Intrathecal Drug Delivery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


