28 Lower Extremity
Lateral Femoral Cutaneous Nerve Block
The clinical description of pain, numbness, and tingling involving the anterior and lateral thigh, was first described by Bernhardt in 1878.1 Werner Hager (1885) was the first to describe compression of the lateral femoral cutaneous nerve near the anterior superior iliac spine (ASIS) as the cause of pain near the hip.2 In 1895, both Bernhardt and Roth published separate articles on meralgia paresthetica (MP).3,4 Roth described five patients with similar symptoms and coined the term “meralgia paresthetica” from the Greek words meros for thigh and algos meaning pain.4
Anatomy of the Lateral Femoral Cutaneous Nerve
The lateral femoral cutaneous nerve (LFCN) is derived from the lumbar plexus and its contribution comes mostly from the L2 and L3 nerve roots.5 The LFCN may derive from various other combinations such as L2 and L3, L1 and L2, or L2 or L3 alone.6 The LFCN appears at the lateral border of the psoas muscle just above the crest of the ilium.5 The nerve then travels laterally and inferiorly across the surface of the iliacus muscle from which it is separated by a thin muscle sheath (Fig. 28-1). Both the nerve and the iliacus muscle are covered with a dense fascial layer called the iliac fascia, which is composed of two layers and the LFCN travels between them.7 The nerve continues its course toward the lateral portion of the inguinal ligament posterior to the deep circumflex iliac artery, which courses parallel to the inguinal ligament beneath the iliac fascia.7 Filho and coworkers found in their cadaver study that the anterior lamina of the iliac fascia and the transversalis fasciae fused to form the iliopubic tract (IPT) and the LFCN courses deep to the IPT and reaches the thigh by passing posterior to the inguinal ligament (IL).7
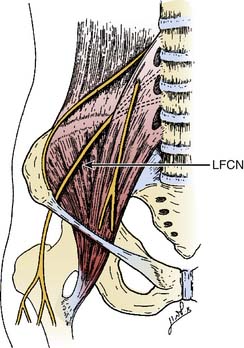
Figure 28-1 The anatomic course of the lateral femoral cutaneous nerve (LFCN).
(Adapted from Mirovsky Y, Neuwirth M: Injuries to the lateral femoral cutaneous nerve during spine surgery. Spine. 2000;25:1266-1269.)
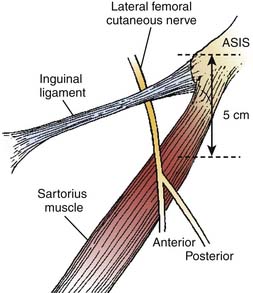
There are several descriptions of anatomic variations of LFCN as it travels from the pelvis to the thigh based on cadaver studies and surgical exploration of the LFCN for meralgia paresthetica.7–12 Keegan and colleagues describes the LFCN as traveling between the two slips of lateral attachment of the IL to the anterior superior iliac spine (ASIS) and remaining just inferior and medial to ASIS.5 It then continues its course anterior to the tendinous origin and upper fibers of the sartorius muscle, separated only by the muscle sheath and covered with the fascia lata. Carai and associates reviewed descriptions of surgical explorations of the LFCN for the treatment of MP and found that in 85.2% of cases the nerve leaves the pelvis beneath the IL (Fig. 28-2).8 This pattern was also documented by Filho and coworkers in their cadaver study where all LFCNs passed posterior to the IL.7 This study also found that in 94% of cases the nerve passed 3.0 cm or less medial to the ASIS.7 Similar results were also described by Grothaus and associates in their cadaver study, in which all the nerves leave under the IL and approximately 36 mm medial to the ASIS.9 Interestingly, they also found that the nerve divides 27.6% of the time before crossing the IL, which may have important implications for nerve blocks or surgical treatment of MP. Aszmann and colleagues in their cadaver study found five variations of the LFCNs as they enter from pelvis to thigh (Fig. 28-3). In 52 cadavers, they found that the nerve overlies the iliac crest 4% (type A), ensheathed by the IL 27% (type B), ensheathed by the tendinous origin of the sartorius muscle 23% (type C), deep to the IL and medial to the sartorius muscle 26% (type D), and 20% of the time the nerve lies medial and on top of the iliopsoas muscle (type E).10 After emerging from the pelvis, the LFCN passes anterior to the tendinous attachment and upper fibers of the sartorius muscle, separated by the muscle sheath and covered by the thick fascia lata.5 Others, however, describe that the nerve may pass over, under, or through the proximal portion of the sartorius muscle.7 Filho and coworkers describes three basic patterns of terminal branching of the LFCN in 26 cadavers.7 The most common pattern (54%) is the bifurcation into anterior and posterior branches (Fig. 28-4). The anterior branch again divides into medial and lateral branches and supplies the anterolateral thigh and the posterior branch supplies the proximal part of the lateral thigh. In a significant number of cases (34%), the nerve divides into medial and lateral branches and supplies the medial and lateral portion of the anterolateral thigh. In 12% of cases, the nerve trifurcates instead of bifurcating. They also observed, in most cases, that the terminal branches, rather than the trunk, pierce the fascia lata to enter the subcutaneous tissues.
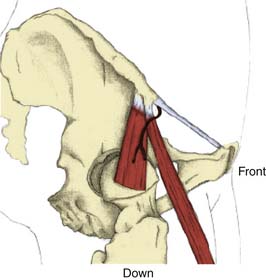
Figure 28-2 Emergence of the nerve from the pelvis under the inguinal ligament.
(Adapted from Carai A, Fenu G, Sechi E, et al: Anatomic variability of the lateral femoral cutaneous nerve: Findings from a surgical series. Clin Anat. 2009;22:365-370.)
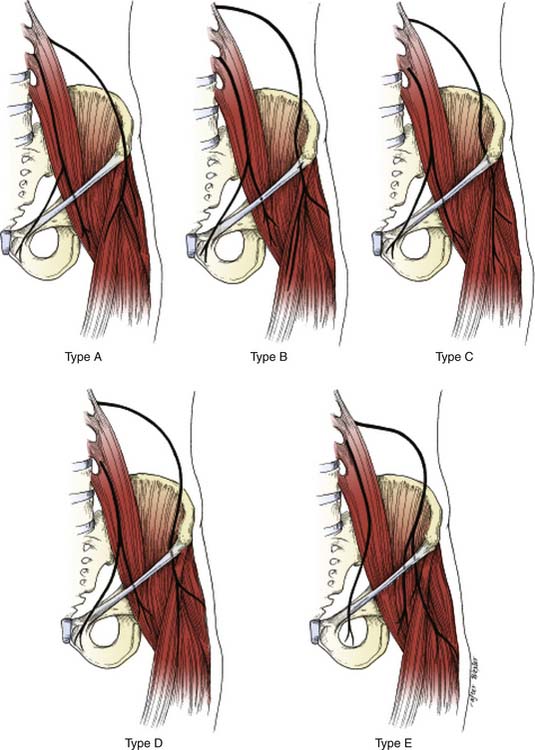
Figure 28-3 Five common variant locations of the LFCN as it exits the pelvis of 52 cadavers (see text for details).
(Adapted from Aszmann OC, Dellon ES, Dellon AL: Anatomical course of the lateral femoral cutaneous nerve and its susceptibility to compression and injury. Plast Reconstr Surg. 1997;100:600-604.)
Etiology
Meralgia paresthetica is a peripheral sensory mononeuropathy of the LFCN. The etiology of MP can be divided into two major categories—spontaneous and iatrogenic (Fig. 28-5). Spontaneous causes include mechanical compression of the nerve or metabolic derangements in the absence of prior surgical procedures that may have injured the nerve. Other mechanical factors include obesity, pregnancy, ascites,12 pelvic tumor,13 tumor in the iliac crest,14 tight trousers,15 corsets, tight belts with accompanying holster for a pistol,16 and soldiers wearing body armor.17 MP has also been described in limb-length discrepancy18 and following the treatment of osteoid sarcoma in children.19
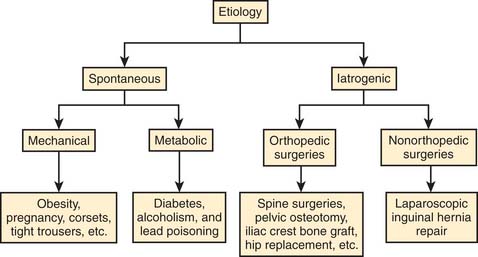
The iatrogenic causes of MP are described after various surgical procedures. This may be caused by direct trauma to the nerve during the procedure, related to patient positioning for the surgery,20 or related to postsurgical scarring.21 The surgical procedures may be classified as orthopedic and nonorthopedic procedures. The orthopedic procedures include pelvic osteotomy,22 acetabular fracture surgery,23 and bone-graft harvesting from the iliac crest.21,24,25 The nonorthopedic surgeries that have been associated with MP are laparoscopic hernia repair,26 laparoscopic cholecystectomy,27 and bariatric surgery.28
Pathophysiology
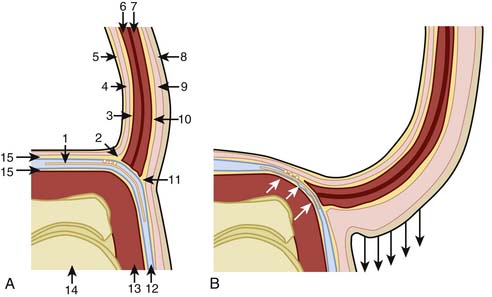
A key factor in the pathogenesis of MP is likely the significant anatomic variation of the nerve described in various cadavers and surgical studies.7–10 Filho and his colleagues,7 in a cadaver study, described the pelvic portion of the LFCN and its relationship with iliac fascia and other muscles and fascia of the anterior abdominal wall. They illustrate that the anterior lamina of the iliac fascia (ALIF) fuses with the transversalis fascia to form the iliopubic tract (IPT) and continues further to meet with the IL. In their study all LFCNs passed inferior to the IPT and were in contact with it (Fig. 28-6). The angle between the ALIF and the IPT becomes more obtuse as the lower abdominal wall moves anteriorly and inferiorly as occurs in obesity (see Fig. 28-4). The authors hypothesized that because the ALIF is firmly attached with the muscles of the abdominal wall, with obesity the ALIF is pushed inferiorly to compress the LFCN. The authors speculated that with erect posture, gravity may further exacerbate the situation by pulling the adipose tissue and the viscera, reflecting the worsening symptoms of patients of MP seen with standing and improving on lying down. Based on their findings of the widening of the LFCN just proximal to the IL, the authors speculate that the nerve may also be compressed within the “LFCN tunnel” (beginning under the IPT and finishing at the IL). It has been found that the groin pressure was greater in sitting obese patients than in subjects with normal weight.29 This becomes more important when the nerve course is close to the ASIS (types A, B, and C, see Fig. 28-3).10 This may increase the likelihood of nerve compression, especially in obese individuals and those with hip extension.10,11
Many researchers suggest that the usual traumatic site for the LFCN is at the IL.5,9,30,31 Keegan and coworkers describe the emergence of the LFCN between the two slips of the lateral attachment that may be affected by the tension of the ligament.5 The authors’ point to the attachment of muscles and fascia and the role they may play with the tension of the ligament. The sartorius muscle has a medial aponeurotic expansion that attaches to the inferior border of the IL and may cause episodic depression of the ligament with muscle contraction. The IL also provides an insertion for the external oblique muscle and an origin for the lowest fibers of the internal oblique and transversus abdominis muscles and thereby create tension by the contraction of these muscles. The deep layer of the superficial abdominal fascia, or Scarpa fascia, extends downward one half inch below the IL to attach with the fascia lata. This attachment with the fascia lata may cause a downward pull of the IL among patients with dependent abdominal fat.5
Diagnosis
Diagnosis of MP is usually done by history and physical examination, with the characteristic location of pain and numbness confined to the anterolateral thigh (Fig. 28-7).32 In rare cases, the area may extend inferiorly below the knee, gluteal region, and medial thigh.12,32
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


