Figure 34.1
Veress needle placement. A Veress needle is placed into the left upper quadrant. After a negative saline drop test, the abdomen is insufflated to a pressure of 15 mmHg

Figure 34.2
Abdominal port positioning. This patient has a 2 cm umbilical hernia. Only 3 ports are needed given that we typically use a small mesh (9 cm round) for this type of hernia. The ports are placed quite lateral both on the right and left side to ensure an adequate working space once the mesh is placed into the abdomen
At least one of the ports is typically a 12 mm port to allow passage of the mesh. If a small piece of mesh is used (e.g., a 9 cm round), an 8 mm port may be used or one of the 5 mm ports may be removed so the mesh can be placed through the port site incision. For most medium sized hernia defects, three ports are placed on the patient’s left so the surgeon can have two working ports on the same side of the abdomen that the camera is located. A single right-sided port is usually necessary for fixation of the mesh along the left margin of the mesh. If this is too difficult with the camera on the left side, an additional 5 mm port can be placed on the patient’s right such that the surgeon is not working opposite the camera.
Dissection and Characterization of Hernia Defect
A combination of blunt and sharp dissection with scissors is used to reduce herniated abdominal contents from the abdominal wall. The most commonly herniated contents are omentum and small bowel although the transverse colon and other organs such as the liver or stomach can be present within the hernia (Fig. 34.3). Tedious dissection is critical during this phase of the operation to avoid the dreaded complication of a missed enteric injury. Our preference is to avoid usage of cautery or bipolar energy devices if possible given the possibility of enteric injury. Often, a combination of gentle pushing and pulling using atraumatic graspers will result in separation of the omentum from the hernia sac. If the omentum is densely adherent to the abdominal wall and cannot be easily reduced, judicious use of cautery or bipolar energy devices is reasonable if we are able to ensure that no bowel is in close proximity. If the anatomy is unclear or we are unable to reduce the herniated contents laparoscopically, we do not hesitate to convert to an open approach to finish the hernia reduction.
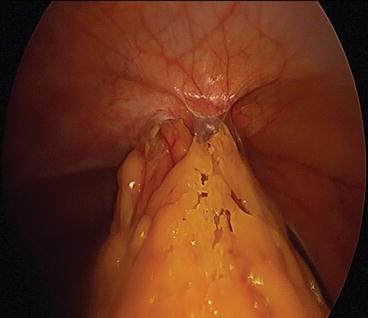
Figure 34.3
Herniated omentum. Herniated omentum can be seen exiting through the umbilical defect while an adhesion can be seen in the foreground. This herniated tissue was easily reduced with blunt dissection using atraumatic graspers. Care was taken to avoid ripping the omentum as this frequently causes bleeding
A plastic ruler is then introduced into the abdomen to measure the length and width of the fascial defect. Two atraumatic graspers are used to stretch the ruler in both the cranial-caudal and lateral directions to abdomen these measurements. We prefer at least 3 cm of overlap between the mesh and fascial edges on each side to minimize the likelihood of hernia recurrence.
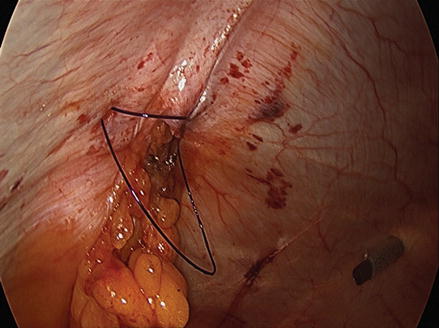
Closure of the Hernia Defect
Given that laparoscopic ventral hernia repairs are typically performed for small to medium sized hernia defects, it is usually possible to close these hernia defects primarily before placing the intra-abdominal mesh. While there is no consensus on whether this maneuver decreases hernia recurrence, it helps decrease the dead space superficial to the intra-peritoneal mesh and closes the hernia defect. To perform this closure, the center of the fascial defect is marked with a pen and a stab incision is made with a 15 blade scalpel. A #1 or 0 suture is then passed transfascially with a suture passer (e.g., Endo CloseTM or Carter-Thomason device) (Fig. 34.4). Multiple sutures can be placed along the fascia from the same skin incision site. This minimizes the number of stab incisions that are needed. For most defects, 2–3 stab incisions are used to pass 5–10 transfascial sutures. Alternatively, the fascia can be sutured closed intracorporeally using a slowly absorbable barbed suture.