Cause
Number
Accidents (unintentional injuries)
12,032
• Motor vehicle accidents
6,984
• All other accidents
5,048
Intentional self-harm (suicide)
4,688
Assault (homicide)
4,508
Malignant neoplasms
1,609
Diseases of the heart
948
Congenital anomalies, deformations and chromosomal abnormalities
429
Influenza and pneumonia
213
Cerebrovascular disease
186
Pregnancy, childbirth and the puerperium
166
Chronic lower respiratory disease
160
All other causes
4,666
Total
29,605
The special discipline of biomechanics that is concerned with injury caused by mechanical interaction is denoted as biomechanics of injuries or trauma biomechanics and is the subject of this book. Since there are a great many types of injuries, injury mechanisms and activities which are prone to cause injury, a large variety of human activities and situations where excessive loads may occur has to be considered. When performing a thorough analysis of such circumstances, however, it becomes evident, that trauma biomechanics is strongly dominated by its interdisciplinary character. First of all, the field of biomechanics itself covers a wide range of areas of interest, from macroscopic motion analysis in sports, for example, to the sub-microscopic modelling of molecular transmembrane transport. Many basic biological aspects are furthermore involved for we are dealing with living matter associated with intrinsic active processes such as muscle contraction or electrochemical activities. The wide-spread knowledge obtained during the recent decades in the different fields covering mechanics and biology in general greatly contributes to trauma biomechanics, in that for an in-depth understanding of injury processes all aspects from the macroscopic scale to the sub-cellular level may have to be taken into account. Therefore, many subjects of importance for trauma biomechanics relating to basic mechanics, anatomy and physiology have to be covered in order to be able to treat the entire field in a systematic approach; nevertheless, in view of the great diversity that exists, a selection has to be made and comprehensiveness is not reached.
1.1 About the Contents of This Book
Several preliminary remarks are useful in order to elucidate the extent and limitations of the subjects treated in this book:
1.
A distinction has to be made between injury resulting from unexpected, sudden and singular events, i.e., accidents in a strict sense, and injury caused by the chronic exposure to unfavourable loads over extended periods of time. A head injury of a pedestrian that is sustained from an impact on the hood of an automobile during a collision, or the gradual destruction of hair cells in the inner ear as the result of a chronic exposure to loud music—both examples are associated with injury, yet, the type of injury, injury mechanisms, tolerance levels, injury criteria, reconstruction and analysis methods as well as protection measures differ fundamentally. Also with respect to insurance and liability issues, procedures are greatly different.
2.
The injury causing period in the course of a traffic accident has a duration of 100–200 ms typically whereby the early part of this period is often decisive. In many cases the person involved is not aware of the event and does not (cannot) react prematurely to the imminent danger. Accordingly, muscular reactions which set in with a time delay of 60–80 ms are often of secondary importance only and can therefore be disregarded. The situation is basically different in case of chronic overloading, where physiological and also psychic reactions are always in the foreground.
3.
A further important aspect is related to age. The mechanical properties of human tissue, organs and body as a whole change, in particular with respect to injury tolerance, decisively during aging towards unfavourable levels. There are a number of reasons for this, among them, a reduction of tissue compliance due to a decrease of body water content along with a stiffening of soft tissue and a gradual demineralization of bone at ages above 30–40 years. As a result, the advent of injury, primarily bone fractures, increases dramatically with age. The incidence even of spontaneous fractures, occurring under normal physiological loads, is well known. In view of the aging population in the industrialized countries, this aspect has to be given particular attention.
4.
Adolescence, at the other end of the age scale, poses likewise important problems for trauma biomechanics in that mechanical and biological properties undergo dramatic changes from birth to adult age. Experiments with children are hardly conceivable; also work with adolescent cadavers is not a routine matter. Downscaling from adult characteristics to children needs a careful analysis (“children are not small adults”). The development of child dummies, in particular (see Sect. 2.6.1) is therefore not straightforward. Due to the lack of experimental approaches, statistics represent the main method for the analysis of child injury. A significant contribution in this direction is made by The Center for Injury Research and Prevention at The Children’s Hospital of Philadelphia (http://injury.research.chop.edu/).
5.
The mechanical response of the body in case of pathological alterations may furthermore be significant. Renal trauma as a result of stress concentration around a cyst has been observed in urology or the aggravation of the effects of a whiplash-type event due to pre-existing neck impairment is a well known complication.
6.
Under very restrictive conditions, however, micro-injury on a cellular level may to some extent be advantageous for tissue regeneration. Figure 1.1 shows the micro callus formation following micro-damage in spongy bone which may serve as an example of an injury that stimulates bone remodelling. After a long and strenuous hiking tour such micro-injuries in the bones of a healthy foot are quite common. Chronic overexposure, in contrast, may lead to quite adverse developments. Figure 1.2 exhibits a marathon runner whose skeleton was largely demineralised due to excessive training.
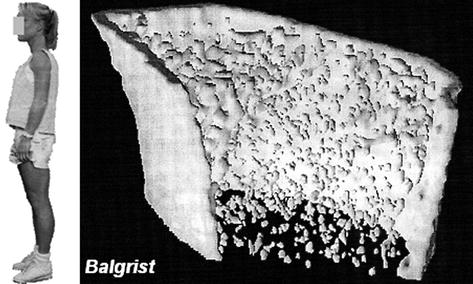
Fig. 1.1
Microcallus formation. The picture exhibits a 3D micro computed tomography (micro CT) scan of the excised portion (biopsy) of a human iliac crest where microfractures induced new bone formation (Courtesy Prof. R. Müller, ETH Zurich)
Fig. 1.2
Twenty-eight year old woman (left) and micro-CT scan (non-invasive) of radius close to the wrist (right). The extreme demineralisation of the radius is to be attributed to excessive training as a Marathon runner (Courtesy Prof. M. Dambacher M.D, Balgrist Orthopaedic Hospital, University of Zurich)
7.
Injuries are suffered mostly in connection with motion (sports, household, etc.) or mobility (traffic). While in general biology the use of animal models (under restrictive regulations) is widespread, the non-linearity inherent in motions and related injury mechanisms prevent scaling up from, say, rats to humans almost completely. Accordingly, except for aspects of basic physiology, only scarce information in trauma biomechanics derives from animal experiments.
8.
When the entire spectrum of “injury” including causation, frequency, prevention, mitigation, rehabilitation, long-term sequelae and socio-economic consequences is considered, clinical medicine cannot be disregarded, since the treatment of injury is made by medical doctors providing in- and outpatient service. It is thereby often forgotten that the overall reduction of specific mortality (i.e., mortality by case) which is observed in most activities associated with a risk of injury, is partly due to dramatic developments of emergency rescue services, first aid procedures and intensive care treatment. A drawback however is that an analysis of injury mechanisms and accidental events is sometimes made by physicians without a complete knowledge of the relevant facts. This may be a consequence of their intense and highly demanding work with patients. Yet, an objective assessment on a scientific basis of the severity and causality aspects of accidents resulting in injuries requires a multidisciplinary approach. In addition to the medical information retrieved by clinicians, all technical and biomechanical circumstances have to be taken into account in accident analysis and reconstruction. This is especially important in cases of forensic expert witnessing. A specialized education and extensive experience is required for this purpose.
9.
This book is primarily focused on the mechanics of injuries which are inflicted without intention. However, injuries may also be conveyed intentionally in a criminal, terroristic, or battlefield environment. Related subjects include wound ballistics, protective garment for soldiers or low-injury producing police weapons. The chapter on ballistic and blast trauma partly includes aspects associated with injuries that exhibit an intentional background. The reader further interested in such issues is referred among others to several publications by the International Committee of the Red Cross (http://www.icrc.org) where also further references can be found. The overall significance of intentional injuries (under non-belligerent circumstances) should in any event not be underestimated; e.g., there were around 11,000 deaths in the US (2010) due to the use of firearms (not including accidental firearm incidents and suicide) in comparison with some 12,000 persons who were killed in the same year as passengers of an automobile. The situation is thereby quite diverse: According to UN statistics, in the United States in 2009, 3.0 intentional homicides committed with a firearm per 100,000 inhabitants were recorded, while the figure for the United Kingdom, for example, was 0.07 per 100,000, about 40 times lower, and for Germany 0.2. Gun homicides in Switzerland are similarly low, at 0.52 in 2010 even though Switzerland ranks third in the world for the number of guns per citizen. Suicide is a further important cause (Table 1.1). Nontechnical aspects (social, political, psychological, general society-related) are particularly important in this context. Investigations, e.g., on the influence of physical violence in childhood (Paradis et al. 2009) involve large-scale socio-psychological cohort analysis.
10.




The least serious injuries are of course those that do not occur. Accordingly, injury prevention is given a high priority in all situations where injury may happen. The prevention of traffic accidents has been recognized and implemented as an important governmental task since decades. In contrast, injury prevention in sports has primarily been perceived by international and national sports associations within the framework of sports medicine, mostly in the form of rigorous regimentation, ban of certain particularly violent variants of sports, development of protective devices such as helmets or shin guards and trainer education. Insurance companies furthermore support all injury prevention campaigns as part of their mission whereby these efforts include especially also workplace and household accidents. While all of these preventive activities are oriented towards pre-accident conditions, extensive rehabilitation is often required after injury has occurred and healed. Again, government agencies, sports federations, professional work associations, clinical medicine as well as insurance companies develop extensive efforts. Since this book is devoted and limited to trauma biomechanics, aspects of prevention and rehabilitation are only included in so far as there is a direct relation with the occurrence of injury.
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
