Fig. 36.1
Magnetic resonance images of an extensive intramedullary tumor in lower thoracic spinal cord with complete obstruction of the spinal canal (a), significant enhancement (b), and dark T2-signal indicating fibrous tissue (c). The large size on imaging does not even allow the differential diagnosis of an intramedullary versus an intradural-extramedullary tumor
Surgery and Intraoperative Monitoring
The monitoring routines for surgery of intramedullary spinal cord tumors include MEP and SSEP recordings from the upper and lower extremities. Thenar, tibialis anterior, flexor hallucis brevis bilaterally were used. Cortical SSEP responses were recorded from median and tibial nerve stimulation. In thoracic tumors, the upper extremity recordings serve as controls for the surgically relevant lower extremity recordings. In addition, recordings of bulbocavernosus reflex, pudendal nerve SSEPs and anal MEPs can be attempted.
The patient was positioned prone with the head in a soft face padding mounted on a mirror plate. During the approach phase of the operation, a sudden drop in the cortical amplitude of the right median nerve was noted (Fig. 36.2). An immediate assessment of the situation showed that unchanged recordings from the left side excluded the possibility of a systemic effect such as a change in anesthesia regimen. The surgery was excluded because the relevant spinal level was low thoracic and therefore not corresponding to the median SSEP. Inspection of the electrodes and cables as well as the patient’s positioning showed an insufficient padding and malposition of the right arm. This was corrected and the recordings normalized at the next set of recordings.
Fig. 36.2
A sudden drop in cortical signal amplitude from the right median nerve SEP prompted analysis and insufficient padding and suboptimal arm position was found and corrected. This resulted in rapid recovery of the response. The contralateral side showed no change at the same time, indicating that it could not be caused by systemic factors
During resection of the spinal cord tumor, significant difficulty was encountered as the tumor was found to be very firm and thus could not be grabbed or easily decompressed. Internal decompression was achieved using a microsurgical laser [34]. This brought the size of the mass sufficiently down so that the remaining tumor mass could be dissected out of the edematous spinal cord in toto. There was no further significant change in either motor- or sensory-evoked potential recordings.
The patient awoke from anesthesia without significant motor deficits. Postoperative MRI showed complete tumor removal.
Case Summary Interpretation and Discussion
A 55-year-old man with progressive paraparesis underwent resection of an intramedullary tumor eventually diagnosed as a solitary fibrous tumor (Fig. 36.1) [35]. During surgery, a unilateral sudden decrease of median nerve SSEP was noted (Fig. 36.2) and found to be caused by less-than-optimal padding of the right forearm. Improved positioning rapidly improved the response. This was a mechanical problem unrelated to the operation per se, due to patient positioning which was identified and corrected immediately.
This case demonstrates that routinely recording evoked potentials from upper and lower extremities is useful even when the surgery takes place caudal to the level of the cervical spinal cord. Upper extremity recordings may serve as controls for difficult lower extremity recordings and as controls to systemic effects of core temperature change and the effects of anesthetic agents. Considering the possible influences of these factors, it became evident that the observed change must have been caused by a nonsurgical (far cranial to the surgery) influence and a nontechnical (no artifacts, correct electrode positions), nonsystemic (stable recordings contralaterally and on the lower extremities) problem. Positioning-related compressive neuropathy is not an infrequent occurrence in complex surgical positioning [36]. Early detection is possible with an evoked potential change such as the one shown here [37]. The case also provides evidence that even SEPs requiring averaging can provide fast information upon potential and correctable problems.
Case 2
History, Clinical Assessment, and Imaging
A 4-year-old boy with nighttime neck pain and progressive clumsiness of the right hand was diagnosed with a cervical intramedullary spinal cord tumor. On MRI, the lesion showed a marked heterogeneity and significant internal compression of the spinal cord by both solid tumor masses and cystic formations (Fig. 36.3). Tumor resection was recommended to obtain a histologic diagnosis and as optimal primary tumor treatment.
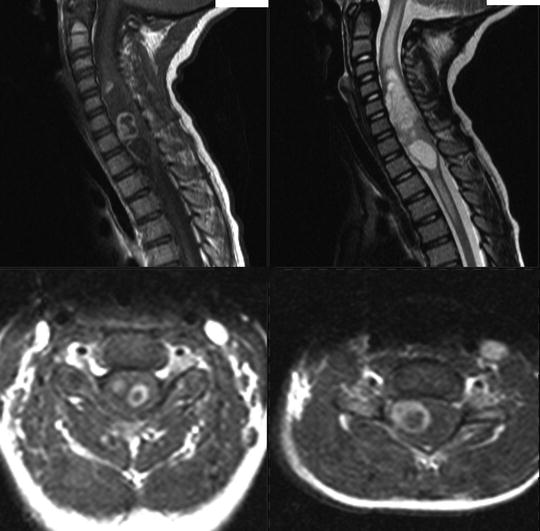
Fig. 36.3
Sagittal and axial MR images of the pilocytic astrocytoma in the cervical spinal cord
Surgery and Intraoperative Monitoring
Routine monitoring for cervical intramedullary spinal cord tumors includes MEP and SSEP recordings from the upper and lower extremities. Thenar, tibialis anterior, flexor hallucis brevis are used. In this context, cortical SSEP responses are recorded from ulnar and tibial nerves, respectively. If possible, an epidural electrode is inserted to record D waves.
The patient was positioned prone with the head fixed in neutral position in a four-pronged Sugita headholder. A laminotomy C3 to T3 was made for surgical exposure. After a dorsal myelotomy , the extensive tumor tissue was removed in piecemeal fashion using the Cavitron ultrasonic aspirator (CUSA), regular suction, and the microsurgical laser. MEP and SEP signals for the entire right side were permanently lost during resection on the right side (Fig. 36.4). Waiting, irrigation, induced hypertension, and additional steroid administration did not achieve recovery of the recordings. The resection remained subtotal. No attempt was made to remove tumor residuals adherent to the still-functioning left side of the cord. The patient awoke with a severe right-sided hemiparesis. Over the long run he recovered motor function of the left side, learned how to walk and run, but remained with a severely impaired right hand and an abnormal gait.
Fig. 36.4
MEP recordings from the right and left hypothenar (bottom traces) and the right tibialis anterior and abductor hallucis muscles, respectively (top traces). The lower extremity recordings disappear simultaneously at a well-defined point. The right hypothenar recordings disappeared gradually and remained stable on the left side
Case Summary Interpretation and Discussion
A 4-year-old boy underwent surgical resection of a cervical intramedullary spinal cord pilocytic astrocytoma . At a critical stage of the resection, a significant change of MEPs of both upper and lower extremities occurred on the right side. MEP and SSEP signals for the entire right side were permanently lost. The resection remained incomplete and the patient had a severe right-sided hemiparesis. The leg recovered partially, the upper extremity remained significantly impaired.
This case demonstrates both the immediate feedback provided by the loss of MEPs on one side and the significant neurologic consequences of a complete loss of both upper and lower extremity recordings. Usually the leg recovers faster and easier than the hand, and unilateral loss of lower extremity MEPs usually recovers completely [14]. However, the complete loss of both extremities on one side appears to have graver consequences. This young patient recovered gross motor function of the arm but not the motor skills adequate for the dominant hand. He developed left-handedness and his rehabilitation was aimed at achieving this goal. His walking improved rapidly to independence but his gait remained massively abnormal.
The preoperative anatomy allowed a preassessment that the right side was under significant risk and that the left side must be preserved at all cost. This concept unfolded during the operation in that indeed the right side suffered, but the left could be preserved and thus useful functioning and social independence was saved. Continuation of the surgery to achieve an anatomically complete resection even of the tumor components involving the left side of the cord would likely have resulted in a complete loss of motor function bilaterally.
Case 3
History, Clinical Assessment, and Imaging
A 54-year-old woman with a year-long progressive history of nighttime back pain presented with a sensory level below Th7 and MR imaging revealed an intradural-extramedullary tumor at the level of Th9 (Fig. 36.5).

Fig. 36.5
Sagittal and axial MR images of what turned out to be a meningioma which was tightly adherent to the pial surface of the spinal cord
Surgery and Intraoperative Monitoring
The monitoring routines for surgery of intradural-extramedullary tumors and intramedullary spinal cord tumors are identical with MEP and SEP recordings from the upper and lower extremities. Thenar, tibialis anterior, flexor hallucis brevis bilaterally were used.
The patient was positioned prone. During the laminectomy, baseline recordings were obtained. Upon opening of the dura, significant hemorrhage occurred from around the tumor and epidurally. Adequate exposure and hemostasis required some time and some blood loss. Left tibialis anterior MEPs disappeared at that time. Blood loss was rapidly compensated with fluid replacement. There was no significant hypotension during that time. MEPs reappeared after about 40 min (Fig. 36.6).
Fig. 36.6
Loss and reappearance of muscle MEPs in the lower extremity on one side during hemorrhage and tumor removal
Summary, Interpretation, and Discussion
A 54-year-old woman underwent laminectomy and resection of an intradural meningioma at T9. This case differs little from intramedullary tumor resections and is therefore presented in this context. After dural opening, a significant hemorrhage occurred. Rapid fluid replacement was considered important and started immediately. Thus, significant hypotension was avoided. Nevertheless, during this time a temporary loss of muscle MEPs from the left tibialis anterior occurred. Both systemic and local factors could have contributed to these findings: local pressure on the tumor and subsequently to the spinal cord during hemostasis and initial tumor resection could have caused temporary MEP loss . In addition, the blood loss compensated through fluid replacement could have contributed to the MEP loss despite stable blood pressure in the situation of both local and systemic vulnerability of the corticospinal system originally due to tumor compression. We consider the proactive maintenance of stable circulatory parameters by the anesthesiologist essential to avoid lasting neurologic dysfunction. It would be an error to wait with fluid replacement until the blood pressure indeed decreases. Correction of the volume deficit at such a late time would be trailing events, carrying more risk for ischemic damage.
Discussion
The use of MEP data, both D wave and muscle MEPs, has found significant acceptance and implementation in the growing community of intraoperative monitoring specialists worldwide. Intramedullary and extramedullary tumors (like the one in Case 3) are basically monitored using the same techniques, practical setups, and interpretation criteria: preservation of muscle MEPs is always associated with preserved motor function, loss of muscle MEPs is highly likely to indicate temporary loss of motor function as long as the D wave is preserved. Loss of both muscle MEPs and D wave is indicating irreversible loss of motor function. There is a scenario of present muscle MEPs but absent or unrecordable D wave. This is interpreted as a desynchronization of the D wave and is sometimes observed in patients with intradural-extramedullary tumors as well as in patients who underwent prior radiation therapy.
Related posts:
 Deep Brain Stimulation
Deep Brain Stimulation
 Intraoperative Neurophysiologic Monitoring During Surgery for Supratentorial Mass Lesions
Intraoperative Neurophysiologic Monitoring During Surgery for Supratentorial Mass Lesions
 Surgery for Chiari Type I Malformation
Surgery for Chiari Type I Malformation
 Intraoperative Neurophysiological Monitoring for Intracranial Aneurysm Surgery
Intraoperative Neurophysiological Monitoring for Intracranial Aneurysm Surgery
 Trigeminal Microvascular Decompression
Trigeminal Microvascular Decompression
 IOM Instrumentation Layout and Electrical Interference
IOM Instrumentation Layout and Electrical Interference
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


