Chapter 44 Hypokalemia and Hyperkalemia
Hypokalemia
8 What are the causes of hypokalemia?
 Redistribution: Intracellular potassium redistribution or shift can be caused by metabolic alkalosis, increased insulin availability, increased β2-adrenergic activity, and periodic paralysis (classically associated with thyrotoxicosis).
Redistribution: Intracellular potassium redistribution or shift can be caused by metabolic alkalosis, increased insulin availability, increased β2-adrenergic activity, and periodic paralysis (classically associated with thyrotoxicosis).
 GI loss: Diarrhea or poor K+ intake.
GI loss: Diarrhea or poor K+ intake.

 Low intake: Poor oral intake or total parenteral nutrition with inadequate potassium supplement.
Low intake: Poor oral intake or total parenteral nutrition with inadequate potassium supplement.
11 What is the diagnostic approach to a patient with hypokalemia?
After eliminating spurious causes (such as leukocytosis), the diagnosis of true hypokalemia can be approached on the basis of urine potassium concentration, systemic acid-base status, urine chloride level, and blood pressure (Fig. 44-1).
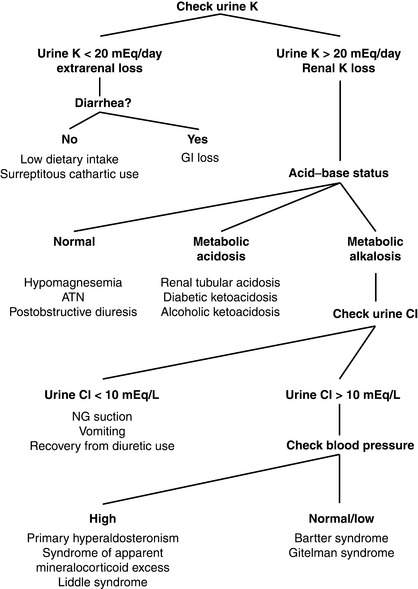
Figure 44-1 Algorithm for diagnosis of hypokalemia. ATN, Acute tubular necrosis; Cl, chloride; NG, nasogastric.
< div class='tao-gold-member'>
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


