Human Immunodeficiency Virus-Related
Human Immunodeficiency Virus-Related
33-1 AIDS-Defining Opportunistic Illnesses
Michael Greenberg
Acquired immunodeficiency syndrome (AIDS)-defining opportunistic illnesses (OIs) include 26 clinical conditions that affect people with advanced human immunodeficiency virus (HIV) disease.
An HIV-infected person receives a diagnosis of AIDS after developing one of the AIDS indicator illnesses defined by the Centers for Disease Control and Prevention (CDC). AIDS-defining OIs are the major cause of morbidity and mortality among persons infected with HIV.
Table 33-1 lists the current CDC-defined OIs.
REFERENCES
www.cdc.gov/hiv/dhap.htm. Last updated 8/9/04.
33-2 Acute HIV Seroconversion Disease
Michael Greenberg
Clinical Presentation
Within 4 weeks after the initial infection with human immunodeficiency virus (HIV)-1, a substantial number of patients develop an acute illness that clinically resembles mononucleosis.
1,
2 This illness is characterized by sore throat, low-grade fever, fatigue, headache, and lymphadenopathy. In addition, an evanescent, faintly red, nonpruritic rash may develop.
1,
2 This rash usually involves the face and tends to have a more central than peripheral distribution. In conjunction with this rash, oral and pharyngeal ulcerations may occur.
Table 33-2 describes some of the clinical and demographic characteristics of one primary HIV cohort.
Pathophysiology
This phase of clinical illness usually lasts 1 to 4 weeks and has been associated with seroconversion for HIV-1 in 53% to 95% of cases.
1,
2
Diagnosis
The diagnosis is made on the basis of information obtained from the history and physical examination. Laboratory findings may include thrombocytopenia, leucopenia, and liver transaminase elevations.
1,
2
Management
Unless the patient is acutely ill enough to warrant hospitalization, the workup may be initiated in the emergency department. This workup includes ruling out intercurrent infection and obtaining relevant baseline laboratory tests, including HIV status testing, CD4-positive T-lymphocyte count, HIV viral load testing, and routine tests. Consultation with an infectious disease specialist should be initiated in the emergency department, because antiretroviral therapy should be initiated as soon as possible.
1,
2
REFERENCES
1. Pederson C, Lindhart B, Jensen B, et al. Clinical course of primary HIV infection: consequences for subsequent course of infection. BMJ 1989;299:154-157.
2. Tindall B, Barker S, Donovan B, et al. Characterization of the acute clinical illness associated with immunodeficiency virus infection. Arch Intern Med 1988;148:945-949.
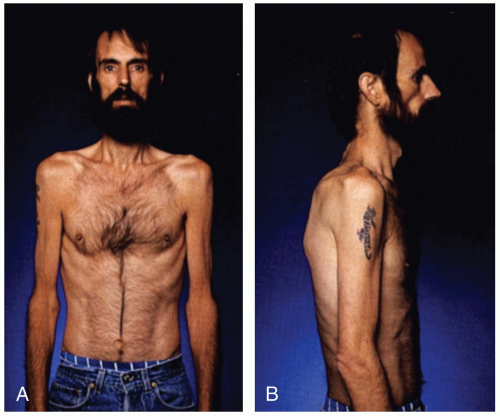
33-3 HIV Wasting Syndrome
Michael Greenberg
Clinical Presentation
HIV wasting syndrome is defined by the Centers for Disease Control and Prevention (CDC) as a weight loss of at least 10% in association with diarrhea or chronic weakness and documented fever for at least 30 days not attributable to conditions other than infection with human immunodeficiency virus (HIV).
1
Pathophysiology
Multiple factors are thought to contribute to the development and propagation of this syndrome. These factors usually represent sequelae of HIV disease, acquired immunodeficiency syndrome (AIDS), or complications thereof and include anorexia, malabsorption, metabolic abnormalities, and hypogonadism.
1 In addition, excessive cytokine production may be associated with wasting and may be partly responsible for the establishment of a vicious cycle of wasting propagated by increased levels of cytokines, which in turn are generated by wasting.
1
Diagnosis
The diagnosis of HIV-related wasting syndrome usually is obvious on observation of the patient, and specific clinical testing usually is not necessary to confirm the diagnosis. However, techniques involving anthropometric measurements, body composition determinations, and nutritional assessments may be helpful for clinicians who care for these patients on a long-term basis. Because treatment of the underlying HIV disease is expected to help control wasting, it is important for emergency physicians to recognize these patients for primary diagnosis, or to facilitate proper treatment and intervention for those who have already been diagnosed.
Clinical Complications
Weight loss related to HIV disease has been associated with the development of acute infections as well as malabsorption.
Management
The emergency physician must determine when and if patients afflicted with wasting syndrome require hospital admission. Clinically important dehydration, weakness, and severe wasting should dictate hospitalization. Physicians who care for these patients over the long term may employ various modalities to correct wasting, including the use of appetite-stimulant drugs, anabolic steroids, growth hormone, and various growth factors. In addition, the drug thalidomide has been shown to increase weight in wasted HIV patients by roughly 4%.
3
REFERENCES
1. Centers for Disease Control and Prevention. Revision of the CDC surveillance case definition of acquired immunodeficiency syndrome. MMWR Morb Mortal Wkly Rep 1987;36:3S-15S.
2. Klausner JD, Makonkawkeyoon S, Akarasewi P, et al. The effect of thalidomide on the pathogenesis of human immunodeficiency virus type I and M. tuberculosis infection. J Acquir Immune Defic Syndr Hum Retrovirol 1996;11:247-257.
3. Cohen PT, Sande MA, Volberding PA, et al. The AIDS knowledge base, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 1999.
33-4 Oropharyngeal Candidiasis
Michael Greenberg
Clinical Presentation
Adult patients with oropharyngeal candidiasis (OPC) present with sore throat, difficulty swallowing, and changes in ability to taste, in conjunction with whitish plaques and deposits on the tongue, oral cavity, and pharynx. Neonates and infants present with excessive crying, poor feeding, and failure to suck properly.
1,
2,
3
Pathophysiology
OPC is found in various patient groups, including those with human immunodeficiency virus (HIV) disease, nutritional deficiencies, or malignancies and those who have undergone organ transplantation, and as a side effect of some medications. Most OPC is caused by overgrowth of
Candida albicans. However, other
Candida species may also be causative of OPC.
3
Diagnosis
The diagnosis is a clinical one. It usually is obvious on visualization of the oral cavity and pharynx.
Clinical Complications
Complications include reoccurrence, intractability, drug resistance, extension to esophageal disease, and systemic candidal infection.
1,
2,
3
Management
Topical fluconazole has been highly effective; however, resistant organisms have emerged. Some cases require systemic antifungal therapy. If candidal disease restricts intake of fluid or food or in any way compromises the airway, hospitalization is essential. Therapy should be initiated for all patients identified in the emergency department; those who are not admitted should be referred for follow-up within 24 hours.
1,
2,
3
REFERENCES
1. Hoppe J. Treatment of oropharyngeal candidiasis and candidal diaper dermatitis in neonates and infants: review and reappraisal. Pediatr Infect Dis 1997;16:885-894.
2. Penzak SR, Gubbins PO. Preventing and treating azole-resistant oropharyngeal candidiasis in HIV-infected patients. Am J Health Syst Pharm 1998;55:279-283.
3. Redding SW. The role of yeasts other than Candida albicans in oropharyngeal candidiasis. Curr Opinion Infect Dis 2001;14:673-677.
33-5 Oral Hairy Leukoplakia
Jason Kitchen
Clinical Presentation
Patients with oral hairy leukoplakia (OHL) present with white thickening of the tongue at the lateral border, with vertical “hairy” projections.
1,
2,
3 Lesions may extend to the tongue’s ventral and dorsal surfaces, where it is usually flat and plaque-like. Lesions can be unilateral or bilateral, and they vary in size from a few millimeters to covering almost the entire surface of the tongue.
1
Pathophysiology
OHL is believed to be an Epstein-Barr virus (EBV)-induced hyperplasia of the upper portions of the epithelial surface of the tongue. No malignant transformation has been identified.
1,
2,
3
Diagnosis
In the HIV-infected patient, the diagnosis is made on clinical appearance. Confirmation can be made by biopsy, and EBV can be demonstrated in lesions.
1,
2,
3 A rapid method for differentiating OHL from oral candidiasis is to wipe the lesions with gauze. In the case of candidiasis, the white plaques can be removed, leaving a tender red base. OHL lesions cannot be removed.
1,
2,
3
Clinical Complications
OHL can become superinfected with
Candida albicans, which can cause soreness and burning. HIV-infected patients presenting with the condition are considered to be at an increased risk for progression to acquired immunodeficiency syndrome (AIDS).
2
Management
Treatment is not needed in most cases. However, OHL regresses in response to acyclovir, ganciclovir, foscarnet, and zidovudine but tends to recur when antiviral drugs are discontinued.
1,
2,
3 Topical application of podophyllum resin has also been used.
1,
2
REFERENCES
1. Patton LL, van der Horst C. Oral infections and other manifestations of HIV disease. Infect Dis Clin North Am 1999;13:879-900.
2. Greenspan JS. Sentinels and signposts: the epidemiology and significance of the oral manifestations of HIV disease. Oral Dis 1997;3[Suppl 1]:S13-S17.
3. Kessler HA, Benson CH, Urbanski P. Regression of oral hairy leukoplakia during zidovudine therapy. Arch Intern Med 1988;148:2496-2497.
Clinical Presentation
Patients with HIV-associated periodontitis (HAP) present with complaints of tooth and gum pain, although some are asymptomatic. Multiple teeth are usually involved, with the anterior, inferior teeth most often affected.
1,
2
33-6 HIV-Associated Periodontitis
Grant Wei
Patients with HIV-associated periodontitis (HAP) present with complaints of tooth and gum pain, although some are asymptomatic. Multiple teeth are usually involved, with the anterior, inferior teeth most often affected.
1,
2
Pathophysiology
HAP is also known as necrotizing ulcerative gingivitis, necrotizing ulcerative periodontitis, or necrotizing stomatitis. It is a necrotic disease of the gums, soft tissues, and bone surrounding the teeth.
1 The incidence of HAP is less than 2% per year.
1 The mixed microflora typically found with the disease is similar to that of classic periodontitis (e.g.,
Porphyromas gingivalis, Prevotella intermedia, Fusobacterium nucleatum). However,
Candida and other anaerobic species (e.g.,
Clostridium, Enterococcus), as well as several viruses, including cytomegalovirus and Ebstein-Barr virus, have also been found in greater numbers of tissue biopsies of HAP, compared with classic periodontitis.
1,
2
Diagnosis
The diagnosis of HAP is made clinically, although HAP is associated with HIV infection early in life, younger age, and with the presence of oral candidiasis. Response to the treatment regimen described here is reported to be near-diagnostic, although wound cultures and tissue biopsy may be required for lesions that do not respond to initial treatment.
1,
2,
3
Get Clinical Tree app for offline access