CHAPTER 73
Hemorrhoids
(Piles)
Presentation
Patients with external hemorrhoids (Figure 73-1) generally complain of a painful anal lump of sudden onset, which may become intense in severity. It will appear to be purple and is located within the anal canal. It may have been precipitated by straining during defecation, heavy lifting, or pregnancy, but, in most cases, there will be no definite preceding event. The external hemorrhoidal swelling is caused by thrombosis of the venous complex. It is very tender to palpation and usually does not bleed unless there is erosion of the overlying skin.
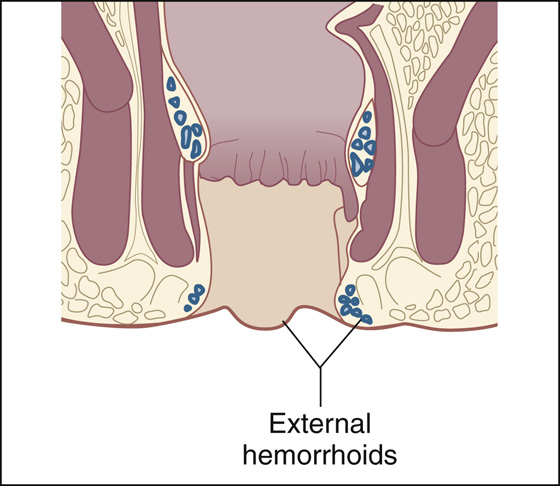
Figure 73-1 External hemorrhoid.
More commonly, patients with internal hemorrhoids (Figure 73-2) usually seek help because of painless (or nearly painless) bright red bleeding during or after defecation. Patients usually notice intermittent spotting on toilet tissue or blood dripping into the toilet bowl, or both. Blood may be admixed with or streaking the stool. A prolapsed internal hemorrhoid appears as a protrusion of painless, moist red tissue covered with rectal mucosa at the anal verge. Prolapsed internal hemorrhoids may become strangulated and thrombosed, and thus painful. Itching is not a common symptom of hemorrhoids.
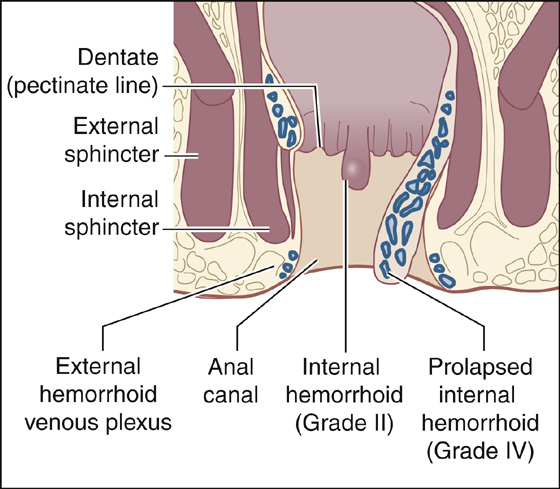
Figure 73-2 Internal hemorrhoid.
What To Do:
 If the problem is rectal bleeding, it should be approached as with any other gastrointestinal (GI) bleeding. The amount of bleeding should be quantified with orthostatic vital signs and a hemoglobin and hematocrit. When there is evidence of severe hemorrhage, rapid volume replacement and early surgical consultation should be initiated.
If the problem is rectal bleeding, it should be approached as with any other gastrointestinal (GI) bleeding. The amount of bleeding should be quantified with orthostatic vital signs and a hemoglobin and hematocrit. When there is evidence of severe hemorrhage, rapid volume replacement and early surgical consultation should be initiated.
 A detailed history will help establish the diagnosis of hemorrhoids. The color and character of anorectal bleeding and any relief the patient may have obtained from reducing a prolapsed hemorrhoid back into the anal canal may lead to the diagnosis.
A detailed history will help establish the diagnosis of hemorrhoids. The color and character of anorectal bleeding and any relief the patient may have obtained from reducing a prolapsed hemorrhoid back into the anal canal may lead to the diagnosis.
 An adequate physical examination should include careful inspection, palpation, and digital examination. Anoscopy and proctosigmoidoscopy should be performed as soon as possible when there is rectal bleeding. However, evidence of hemorrhoidal bleeding does not exclude other causes of rectal bleeding; therefore a complete colonic evaluation should be done at some point in those who are at a risk, based on family history, or who are at an age for colonic screening evaluation. Young patients in whom hemorrhoids are the obvious source of bleeding may not require more than a digital rectal examination and anoscopy.
An adequate physical examination should include careful inspection, palpation, and digital examination. Anoscopy and proctosigmoidoscopy should be performed as soon as possible when there is rectal bleeding. However, evidence of hemorrhoidal bleeding does not exclude other causes of rectal bleeding; therefore a complete colonic evaluation should be done at some point in those who are at a risk, based on family history, or who are at an age for colonic screening evaluation. Young patients in whom hemorrhoids are the obvious source of bleeding may not require more than a digital rectal examination and anoscopy.
 For nonthreatening rectal bleeding from hemorrhoids, the initial management should include a high-fiber diet, stool softeners, and bulk laxatives, and the patient should be instructed to spend less time sitting and straining on the commode. Patients also should be taught not to neglect their first urge to defecate; those who are troubled with constipation should be given an osmotic laxative (see Chapter 67).
For nonthreatening rectal bleeding from hemorrhoids, the initial management should include a high-fiber diet, stool softeners, and bulk laxatives, and the patient should be instructed to spend less time sitting and straining on the commode. Patients also should be taught not to neglect their first urge to defecate; those who are troubled with constipation should be given an osmotic laxative (see Chapter 67).
 Prolapsed or strangulated hemorrhoids warrant surgical consultation and possible hospital admission.
Prolapsed or strangulated hemorrhoids warrant surgical consultation and possible hospital admission.
 If the problem is mild pain, the rectum should be examined using a topical anesthetic (lidocaine jelly) as a lubricant. First, look for thrombosed external hemorrhoids and prolapsed internal hemorrhoids. Have the patient perform a Valsalva maneuver as you provide traction on the skin of the buttocks to evert the anus. Examine the posterior mucosa for anal fissures. After the topical anesthesia has taken effect, complete the digital rectal examination, looking for evidence of rectal abscesses or other masses. Internal hemorrhoids are usually not palpable unless they have prolapsed.
If the problem is mild pain, the rectum should be examined using a topical anesthetic (lidocaine jelly) as a lubricant. First, look for thrombosed external hemorrhoids and prolapsed internal hemorrhoids. Have the patient perform a Valsalva maneuver as you provide traction on the skin of the buttocks to evert the anus. Examine the posterior mucosa for anal fissures. After the topical anesthesia has taken effect, complete the digital rectal examination, looking for evidence of rectal abscesses or other masses. Internal hemorrhoids are usually not palpable unless they have prolapsed.
 If topical mucosal anesthetic does not give enough relief to permit examination, follow with subcutaneous injection of 5 to 10 mL of 1% lidocaine with epinephrine or bupivacaine 0.5% with epinephrine for extended pain relief.
If topical mucosal anesthetic does not give enough relief to permit examination, follow with subcutaneous injection of 5 to 10 mL of 1% lidocaine with epinephrine or bupivacaine 0.5% with epinephrine for extended pain relief.
 If topical anesthetics on the rectal mucosa help control the pain, provide for more of the same, perhaps also with some added corticosteroid for anti-inflammatory effect (Anusol-HC cream). Suppositories are convenient but may not deliver the medication where it is needed; so, prescribe cream or foam (Proctofoam-HC) applied externally rather than internally.
If topical anesthetics on the rectal mucosa help control the pain, provide for more of the same, perhaps also with some added corticosteroid for anti-inflammatory effect (Anusol-HC cream). Suppositories are convenient but may not deliver the medication where it is needed; so, prescribe cream or foam (Proctofoam-HC) applied externally rather than internally.
 Pain may also be relieved by reducing sphincter spasm. Prescribe topical nifedipine 0.2% or diltiazem gel 2% with lidocaine gel 1.5% to be applied every 12 hours. Topical glyceryl trinitrate 0.2% or nitroglycerin ointment can be substituted for the diltiazem and nifedipine, but many patients are unable to tolerate the headaches that frequently occur. (These prescriptions often need to be filled at a compounding pharmacy.)
Pain may also be relieved by reducing sphincter spasm. Prescribe topical nifedipine 0.2% or diltiazem gel 2% with lidocaine gel 1.5% to be applied every 12 hours. Topical glyceryl trinitrate 0.2% or nitroglycerin ointment can be substituted for the diltiazem and nifedipine, but many patients are unable to tolerate the headaches that frequently occur. (These prescriptions often need to be filled at a compounding pharmacy.)
 Instruct the patient to treat lesser pain and itching with witch hazel compresses, a low potency steroid cream, good anal hygiene, and ice packs followed by warm sitz baths or hot compresses. Sitz baths may be the most effective of these therapies; it consists of a warm-water (40° C) bath that relieves tissue edema and sphincter spasm. Zinc oxide paste or petroleum jelly may ease defecation and soothe itching. Prevent constipation by using bulk laxatives (i.e., bran, methylcellulose, polycarbophil) (see Chapter 67) and stool softeners (docusate [Colace], 50 to 100 mg qd), and arrange follow-up. Inform the patient that hemorrhoids may recur and require surgical removal.
Instruct the patient to treat lesser pain and itching with witch hazel compresses, a low potency steroid cream, good anal hygiene, and ice packs followed by warm sitz baths or hot compresses. Sitz baths may be the most effective of these therapies; it consists of a warm-water (40° C) bath that relieves tissue edema and sphincter spasm. Zinc oxide paste or petroleum jelly may ease defecation and soothe itching. Prevent constipation by using bulk laxatives (i.e., bran, methylcellulose, polycarbophil) (see Chapter 67) and stool softeners (docusate [Colace], 50 to 100 mg qd), and arrange follow-up. Inform the patient that hemorrhoids may recur and require surgical removal.
 Small ulcerated external hemorrhoids usually do not require any treatment for hemostasis. Bulk laxatives and gentle cleansing are generally all that is required. Occasionally, patients present several days after an external hemorrhoid has thrombosed with a small gush of dark blood because of a ruptured pile. This may continue to ooze for a day or two. With or without rupture, if the pain has subsided, all that is required is reassurance and the general measures described previously. Inform the patient that symptoms should resolve in approximately 2 weeks.
Small ulcerated external hemorrhoids usually do not require any treatment for hemostasis. Bulk laxatives and gentle cleansing are generally all that is required. Occasionally, patients present several days after an external hemorrhoid has thrombosed with a small gush of dark blood because of a ruptured pile. This may continue to ooze for a day or two. With or without rupture, if the pain has subsided, all that is required is reassurance and the general measures described previously. Inform the patient that symptoms should resolve in approximately 2 weeks.
 When an acutely thrombosed hemorrhoid is engorged and causing severe pain, and there are no anticipated bleeding problems, the hemorrhoid should be incised to provide pain relief. Consider using procedural sedation (see Appendix E). Apply an ice pack for 15 minutes; then, using the smallest needle available, inject around it and infiltrate the dome of the mass with a local anesthetic to allow for examination and excision. As described previously, use lidocaine or bupivacaine with epinephrine. Have an assistant spread the buttocks. The thrombus may be enucleated through an elliptic incision over the anal mucosa. Make the elliptic incision around the clot but not past the cutaneous layer or past the anal verge. Locular clots can be broken up by inserting a straight hemostat into the wound and spreading the tips, thereby allowing the clots to be expressed. Pain relief from this simple surgical technique can be dramatic, but excision is not effective unless the entire thrombosed lesion is completely removed (Figures 73-3 and 73-4). Apply a compression dressing and tape the buttocks together for 12 hours to minimize bleeding. Occasionally, Gelfoam may be needed to help control oozing. The patient can then begin the nonsurgical treatment described previously. Schedule a follow-up examination in 2 days. Narcotics may be prescribed for a few days but should be switched to nonsteroidal anti-inflammatory drugs (NSAIDs) as soon as the risk of bleeding has lessened so as not to cause constipation.
When an acutely thrombosed hemorrhoid is engorged and causing severe pain, and there are no anticipated bleeding problems, the hemorrhoid should be incised to provide pain relief. Consider using procedural sedation (see Appendix E). Apply an ice pack for 15 minutes; then, using the smallest needle available, inject around it and infiltrate the dome of the mass with a local anesthetic to allow for examination and excision. As described previously, use lidocaine or bupivacaine with epinephrine. Have an assistant spread the buttocks. The thrombus may be enucleated through an elliptic incision over the anal mucosa. Make the elliptic incision around the clot but not past the cutaneous layer or past the anal verge. Locular clots can be broken up by inserting a straight hemostat into the wound and spreading the tips, thereby allowing the clots to be expressed. Pain relief from this simple surgical technique can be dramatic, but excision is not effective unless the entire thrombosed lesion is completely removed (Figures 73-3 and 73-4). Apply a compression dressing and tape the buttocks together for 12 hours to minimize bleeding. Occasionally, Gelfoam may be needed to help control oozing. The patient can then begin the nonsurgical treatment described previously. Schedule a follow-up examination in 2 days. Narcotics may be prescribed for a few days but should be switched to nonsteroidal anti-inflammatory drugs (NSAIDs) as soon as the risk of bleeding has lessened so as not to cause constipation.
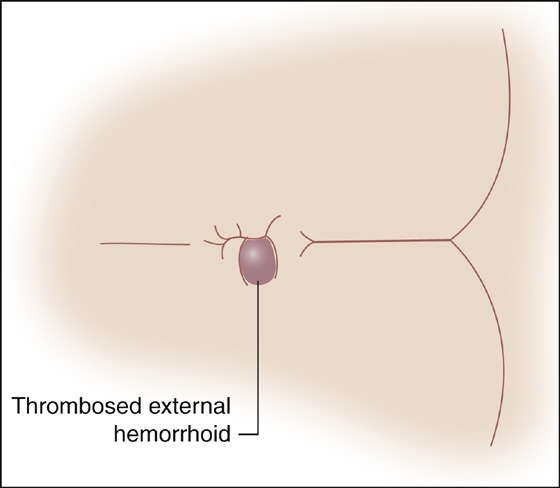
Figure 73-3 Thrombosed external hemorrhoid.
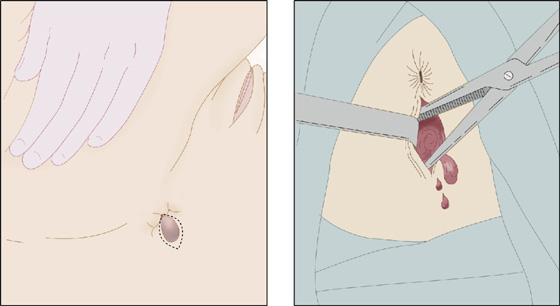
Figure 73-4 Thrombosed hemorrhoid excision.
What Not To Do:
 Do not labor to reduce prolapsed hemorrhoids unless they are part of a large rectal prolapse with some strangulation. Everything may prolapse again when the patient stands or strains. Bulky but asymptomatic hemorrhoids should be left alone. Treatment is directed toward symptom control, not appearance, until definitive care is received.
Do not labor to reduce prolapsed hemorrhoids unless they are part of a large rectal prolapse with some strangulation. Everything may prolapse again when the patient stands or strains. Bulky but asymptomatic hemorrhoids should be left alone. Treatment is directed toward symptom control, not appearance, until definitive care is received.
 Do not traumatize the patient when doing an examination.
Do not traumatize the patient when doing an examination.
 Do not miss infectious, neoplastic, and other anorectal pathologic conditions that can resemble or coexist with hemorrhoids. Consider rectal prolapse, polyps, carcinoma, hypertrophied anal papilla, skin tags, fissure, fistula, and perianal abscess in the differential diagnosis.
Do not miss infectious, neoplastic, and other anorectal pathologic conditions that can resemble or coexist with hemorrhoids. Consider rectal prolapse, polyps, carcinoma, hypertrophied anal papilla, skin tags, fissure, fistula, and perianal abscess in the differential diagnosis.
 Do not excise a thrombosed hemorrhoid when the patient has a bleeding abnormality, is taking an anticoagulant or daily aspirin, or has increased portal venous pressure.
Do not excise a thrombosed hemorrhoid when the patient has a bleeding abnormality, is taking an anticoagulant or daily aspirin, or has increased portal venous pressure.
 Do not allow patients to use hydrocortisone topical therapy for longer than 7 to 10 days. Prolonged use can lead to mucosal atrophy.
Do not allow patients to use hydrocortisone topical therapy for longer than 7 to 10 days. Prolonged use can lead to mucosal atrophy.
 Do not have the patient sit on a doughnut-shaped cushion. This may actually increase venous congestion.
Do not have the patient sit on a doughnut-shaped cushion. This may actually increase venous congestion.
Discussion
The word hemorrhoid comes from the Greek hemo (blood) plus rrhoos (flowing). The word “piles” comes from the Latin pila, or ball. As a disease entity, hemorrhoids have been reported to plague the human race since the earliest history of man.
Three quarters of Americans have hemorrhoids at some time in their lives. Predisposing factors include heredity, age, portal hypertension, anal sphincter tone, occupation, low-fiber diet, obesity, diarrhea, straining to defecate, and pregnancy.
The submucosal tissue within the anal canal is made up of a discontinuous series of vascular cushions that contribute to continence by partially occluding the anus. The three main cushions are found in the left lateral, right anterior, and right posterior positions. These vascular cushions may also protect the anal canal from injury by filling with blood during defecation. The deterioration of supporting tissue to the vascular cushions in the anal canal produces venous distention, erosion, bleeding, and thrombosis. Several theories have been postulated regarding the etiology of hemorrhoids; however, the precise cause is still unknown.
Hemorrhoids are classified according to location and degree of prolapse. The dentate line separates internal from external hemorrhoids. Internal hemorrhoids arise proximal to the dentate line and are covered by mucosa. External hemorrhoids are located distal to the dentate line and are covered by squamous epithelia that contain numerous somatic pain receptors. External skin tags, which represent residual excess skin associated with previous thrombosis of external hemorrhoids, or which can be associated with anal fissures or Crohn disease, are often confused with external hemorrhoids, but they are not hemorrhoids.
There is no widely used classification system for grading external hemorrhoids, but internal hemorrhoids are graded from I to IV. First-degree internal hemorrhoids do not protrude, cannot be palpated by digital examination, and require anoscopy for diagnosis. Second-degree hemorrhoids protrude with straining or defecation but reduce spontaneously. Third-degree hemorrhoids prolapse with straining or defecation and require manual reduction. Fourth-degree hemorrhoids are irreducibly prolapsed and may strangulate.
External hemorrhoids are usually small, do not itch, and cause pain only when they are acutely thrombosed. Internal hemorrhoids are usually painless, and patients generally present with painless bleeding or a bloody mucoid discharge, often associated with their prolapse, anal soiling, and, occasionally, pruritus.
Elastic banding techniques, which have become one of the most frequently applied methods of treatment of internal hemorrhoids, can be 80% to 90% curative for second-, third-, and fourth-degree lesions. This technique is associated with a low complication rate (<2%). Patients with bleeding diatheses, or both internal and external hemorrhoids, are best treated by means of surgical resection.
The diagnosis of hemorrhoids may cover a variety of minor ailments of the anus that may or may not be related to the hemorrhoidal veins (vascular cushions). Anal and perianal itching can be caused by dermatologic conditions, such as psoriasis, eczema, lichen planus, and allergic dermatitis (see discussion of pruritus ani, p. 243). Infections of the anal and perianal area include herpes simplex, scabies, candidiasis, erythrasma, and pinworms (see Chapter 69). Perianal itching can also be the result of diabetes, leukemia, aplastic anemia, thyroid disease, hyperbilirubinemia, and precancerous and cancerous lesions. Punch biopsy may be indicated when pruritus ani is chronic.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


