 An estimation of cardiovascular function based on the physical examination and standard hemodynamic data such as blood pressure, central venous pressure, and urine output may be discordant from measured values of cardiac function, cardiac output, and tissue oxygenation.
An estimation of cardiovascular function based on the physical examination and standard hemodynamic data such as blood pressure, central venous pressure, and urine output may be discordant from measured values of cardiac function, cardiac output, and tissue oxygenation. The complementary use of hemodynamic monitoring technology enables the clinician to make a more timely and accurate assessment of cardiovascular function.
The complementary use of hemodynamic monitoring technology enables the clinician to make a more timely and accurate assessment of cardiovascular function. It is imperative to know the advantages and limitations of the monitoring modalities deployed.
It is imperative to know the advantages and limitations of the monitoring modalities deployed. Hemodynamic monitoring enables the clinician to assess cardiopulmonary function and tissue oxygenation.
Hemodynamic monitoring enables the clinician to assess cardiopulmonary function and tissue oxygenation. One of the tenets of critical care medicine is to ensure adequate tissue oxygenation. This determination is often based on the physical examination and the interpretation of standard hemodynamic parameters such as blood pressure, central venous pressure (CVP), and urine output. However, studies have demonstrated significant discordance between assessments based on these parameters and those based on measurements of cardiac function, cardiac output (CO), and tissue oxygenation (1,2,3,4,5,6,7,8). The pediatric intensivist must appreciate that no single observation or measurement taken in isolation can provide adequate hemodynamic monitoring. Rather, it is the application of a range of observations and measurements that allows the care team to balance oxygen delivery with the child’s metabolic demands. The type and intensity of hemodynamic monitoring should be calibrated to prevent tissue hypoxia episodes and, when necessary, to document that adequate tissue oxygenation has been restored.
One of the tenets of critical care medicine is to ensure adequate tissue oxygenation. This determination is often based on the physical examination and the interpretation of standard hemodynamic parameters such as blood pressure, central venous pressure (CVP), and urine output. However, studies have demonstrated significant discordance between assessments based on these parameters and those based on measurements of cardiac function, cardiac output (CO), and tissue oxygenation (1,2,3,4,5,6,7,8). The pediatric intensivist must appreciate that no single observation or measurement taken in isolation can provide adequate hemodynamic monitoring. Rather, it is the application of a range of observations and measurements that allows the care team to balance oxygen delivery with the child’s metabolic demands. The type and intensity of hemodynamic monitoring should be calibrated to prevent tissue hypoxia episodes and, when necessary, to document that adequate tissue oxygenation has been restored.exhibit this pattern, the core-peripheral temperature gradient neither correlates well with other hemodynamic measurements nor predicts circulatory collapse (2,11).
preferred method in smaller children due to improved accuracy of volume infused, which should be taken into account when calculating fluid balance. Infusion sets should be renewed every 72 hours to minimize line infections.
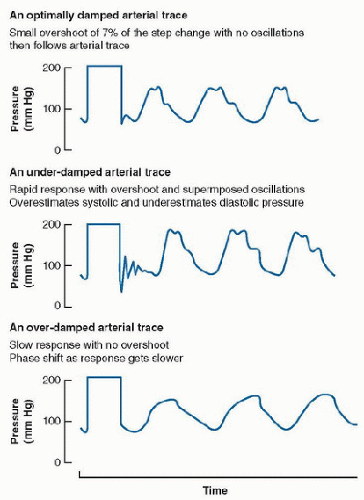 FIGURE 71.1. Quantification of the degree of damping via the fastflush test. Reproduced from Anaesthesia UK web site http://www. frca.co.uk/article.aspx?articleid=100382, with permission. Accessed October 12, 2014. |
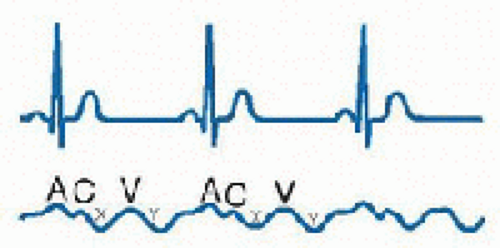
positive and two negative waves: the “a” wave follows the p wave on the ECG and is produced by atrial contraction; the “c” wave is produced by ventricular contraction and bulging of the tricuspid valve upward into the RA; the “x” descent results from atrial relaxation; the “v” wave results from right atrial filling and occurs in late systole before opening of the tricuspid valve; and the “y” descent results from opening of the tricuspid valve and passive filling of the right ventricle (RV). The CVP is the mean right atrial pressure, which approximates the right ventricular end-diastolic pressure, when right ventricular compliance and tricuspid valve function are normal. When ventricular function and compliance are diminished, atrial systole generates an end-diastolic pressure (reflected in the “a” wave) that is disproportionately higher than the mean pressure (14). Cannon “a” waves are produced when right atrial contraction occurs against a closed tricuspid valve, as in atrioventricular disassociation. Prominent “v” waves may be seen in tricuspid insufficiency and rapid “x” and “y” descents are suggestive of pericardial disease and restraint.
 FIGURE 71.2. Arterial pulse waveform. Inspection of the arterial pulse waveform provides a first approximation of various aspects of hemodynamic function. The slope of the systolic upstroke may be proportional to myocardial contractility and inversely proportional to systemic vascular resistance. The area under the systolic curve approximates stroke volume. The duration of systole relative to the duration of the entire cardiac cycle reflects myocardial O2 demand. The duration of diastole relative to the duration of the entire cardiac cycle reflects myocardial O2 supply. Pulse pressure is the difference between systolic and diastolic pressures. |
 |
 Ventricular compliance is the ratio of the change of ventricular pressure (ΔP) to the change in ventricular volume (ΔV). One of the challenges of relying on the central venous (or ventricular filling) pressure as an indication of ventricular volume is that the relationship between volume and pressure (i.e., compliance) for a distensible chamber varies considerably from moment to moment in patients with cardiopulmonary disease (15). The effective compliance of the ventricle is affected by pericardial pressure and intrathoracic pressure. Thus, the end-diastolic transmural pressure (ventricular pressure-pericardial pressure) and ventricular compliance are the determinants of ventricular end-diastolic volume (Fig. 71.4). With a decrease in compliance, a greater distending pressure is needed to maintain ventricular filling. Ventricular compliance may be diminished as result of:
Ventricular compliance is the ratio of the change of ventricular pressure (ΔP) to the change in ventricular volume (ΔV). One of the challenges of relying on the central venous (or ventricular filling) pressure as an indication of ventricular volume is that the relationship between volume and pressure (i.e., compliance) for a distensible chamber varies considerably from moment to moment in patients with cardiopulmonary disease (15). The effective compliance of the ventricle is affected by pericardial pressure and intrathoracic pressure. Thus, the end-diastolic transmural pressure (ventricular pressure-pericardial pressure) and ventricular compliance are the determinants of ventricular end-diastolic volume (Fig. 71.4). With a decrease in compliance, a greater distending pressure is needed to maintain ventricular filling. Ventricular compliance may be diminished as result of:
myocardial disease (hypertrophic or ischemic myocardium);
elevated operating volumes, as occurs in systolic heart failure and elevated afterload;
pericardial disease;
an increase in intrathoracic pressure, as occurs with positive pressure ventilation, lower airway disease, and excessive lung volumes;
large pleural effusions.
pressures exceed right ventricular pressures. If the interventricular septum shifts from its normal position, either due to an increase in right or left ventricular diastolic pressure, the compliance and therefore pressure and volume (filling) of the contralateral ventricle is altered.
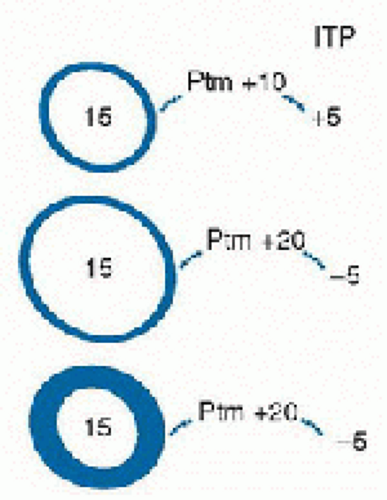 FIGURE 71.4. The pressure-volume relationship for a distensible/collapsible chamber. The degree to which a chamber undergoes deformation depends on its compliance and the magnitude and direction of the pressure exerted across its wall or its transmural pressure (Ptm). The pressure within each chamber is constant at 15. For the top chamber, the surrounding pressure of 5 produces a distending Ptm of +10. The middle chamber, with identical compliance to the top chamber (same thickness), distends to a greater extent because it is surrounded by a negative pressure of 5, resulting in a transmural pressure of +20. The bottom chamber is less compliant than the top two chambers. Even though its transmural pressure is identical to the middle chamber, its volume is less. |
TABLE 71.1 COMMON HEMODYNAMIC VARIABLES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


