Heart Problems
Fredrick Z. Bierman MD
INTRODUCTION
Successful management of heart problems in the pediatric population depends on timely diagnosis and initiation of appropriate medical or surgical intervention. While most practitioners are familiar with congenital and acquired pediatric cardiovascular anomalies, the confounding variability in their clinical presentation is an ongoing challenge. The intent of this chapter is to provide a guideline for pediatric primary care practitioners confronting the varied presentations of infants with congenital heart disease, well children with murmurs, children and adolescents with chest pain or syncope, and patients with acute rheumatic fever (ARF).
CONGENITAL HEART DISEASE IN INFANTS
Cardiovascular examination of the newborn begins with assessment of respiratory status, oxygenation, and exercise tolerance. Tachypnea, cyanosis, and feeding performance are nonspecific parameters of cardiopulmonary physiology in the newborn. During the first month of life, clinicians, either in the nursery or the office, use auscultation to identify systolic and diastolic murmurs and to assess ventilation; palpation to evaluate peripheral perfusion and hepatic size; pulse oximetry to quantitate systemic saturation and saturation gradients; and chest x-ray to assess cardiac size, abdominal viscera laterality, and pulmonary parenchyma. Clinicians must recognize that murmurs are not a universal finding with either simple or complex cardiovascular anomalies. Normal variations or coexisting pulmonary disease can distort the chest x-ray, particularly in neonates.
Pathology
Murmurs reflect pressure gradients across anatomic partitions (interventricular septum), cardiac valves and vascular channels (ductus arteriosus, coarctation), or simply turbulent blood flow. While the absence of a murmur suggests that the interatrial or interventricular septum is intact and the cardiac valves and great vessels are normal, their absence in the neonate does not exclude clinically important cardiovascular anomalies. The limitations of the physical examination and alternative diagnostic resources available to practitioners are illustrated in the following clinical scenarios:
Interventricular septal defect (VSD)
Tetralogy of Fallot (TOF)
Left heart obstructive anomalies
Meconium aspiration with persistence of fetal circulation
Interventricular Septal Defect
The murmur of VSD depends on a pressure gradient between the right and left ventricles. Pulmonary artery pressure at systemic levels in utero declines over the first few weeks of life, with thinning of the muscular wall of the smaller pulmonary arterioles. When right ventricular pressures drop below left-sided pressures, left-to-right shunting occurs across the septal defect, creating the characteristic holosystolic murmur. The appearance of a VSD murmur depends on the rapidity of this vascular maturation process.
• Clinical Pearl
The classic pansystolic murmur of a VSD may not become apparent until after a newborn has been discharged home.
During the perinatal period, the size of the communication, coexisting right ventricular outflow obstruction, or persistence of fetal-type cardiopulmonary circulation may mute audibility of the VSD. The clinical course of most VSDs, particularly those located in the muscular segment of the interventricular septum, is often benign. As the duration and intensity of the systolic murmur decrease on serial follow-up, uncomplicated spontaneous closure of the VSD usually follows.
Complications
Infrequently, spontaneous closure of a VSD may lead to undesirable changes in intracardiac anatomy or pulmonary physiology. Closure of VSDs, particularly those in the subaortic membranous septum, normally is accomplished with fibrous thickening of the defect’s border or adjacent septal tricuspid valve leaflet and formation of a windsock-like aneurysm on the right septal surface. Undesirable herniation of an aortic cusp into the septal defect, however, may initiate closure. In this sequence, the aortic cusp seals the communication, but secondary distortion of the valve results in aortic regurgitation.
• Clinical Pearl
As the VSD systolic murmur decreases in intensity and duration, a pandiastolic, high-frequency murmur of aortic insufficiency becomes audible with herniation of the aortic cusp.
Another variation in the natural history of the relatively small membranous VSD is the spontaneous development of anomalous muscle bundles in the right ventricle. As the VSD spontaneously decreases in size, muscle bundles within the body of the right ventricle hypertrophy, partitioning the chamber into higher and lower pressure segments. The softer systolic murmur of the closing VSD becomes obscured by a harsh ejection murmur. This murmur results from the intraventricular pressure gradient that the anomalous muscle
bundles generate. While the left-to-right shunt is not a hemodynamic burden, surgical intervention in the toddler or younger child may be necessary to resect the obstructing anomalous muscle bundles.
bundles generate. While the left-to-right shunt is not a hemodynamic burden, surgical intervention in the toddler or younger child may be necessary to resect the obstructing anomalous muscle bundles.
Undesirable changes in pulmonary vascular physiology may simulate spontaneous closure of a VSD. While timely surgical intervention during infancy has reduced the frequency of this clinical problem, certain patients experience accelerated maladaptive changes in the pulmonary arterioles in response to increased pulmonary blood flow due to moderate or large VSDs. The media of the arterioles thicken, increasing pulmonary artery pressure and pulmonary vascular resistance. In addition, this thickening reduces left-to-right shunting across the VSD. The pansystolic VSD murmur recedes as right and left ventricular pressures equilibrate, and the left-to-right intracardiac shunt is minimized. Subsequent physical examination reveals no systolic or diastolic murmur. The second heart sound (S2) increases in intensity, and a palpable right ventricular impulse is apparent.
Interventricular Septal Defect as Part of Atrioventricular Canal Defect
In neonates with trisomy 21, a complete common atrioventricular (AV) canal defect (unrestrictive atrial septal defect [ASD], VSD, mitral and tricuspid valve anomalies) may be clinically silent during their physical examination. The pansystolic murmur, which results from left-to-right shunting, is blunted until pulmonary vascular maturation reduces pulmonary vascular resistance and right ventricular pressure. Therefore, newborns with Down syndrome require more than just a careful physical examination. Screening for an AV canal, also known as an endocardial cushion defect, begins with the standard 12-lead electrocardiogram (ECG). In most cases, the neonatal ECG is too nonspecific to identify cardiovascular anomalies; however, the superior QRS axis and counterclockwise depolarization loop associated with an AV canal is characteristic for this anomaly. As with other cardiovascular anomalies whose clinical expression depends on maturation of pulmonary circulation, exclusion of an AV canal anomaly or more complex interventricular septal communications warrants cardiac ultrasound examination.
Tetralogy of Fallot
Although listening for a murmur is a common focus of the practitioner’s assessment when screening for newborn cardiovascular anomalies, TOF illustrates how variable such findings may be. The anomalies in TOF consist of a large malalignment-type VSD; an aortic valve overriding the interventricular septum; obstruction of the pulmonary circulation below, at, or above the pulmonary valve; and right ventricular hypertrophy. Although a large VSD is part of the complex, it does not typically contribute to the auscultatory findings in an affected neonate. The systolic ejection murmur at the left upper sternal border associated with TOF is secondary to the obstruction and attendant pressure gradient across the right ventricular outflow tract.
Variations in the auscultatory findings in TOF reflect the dynamic and static nature of the right ventricular outflow tract obstruction. Patients vary in the degree of fixed obstruction across the hypertrophied, right ventricular outflow, stenotic pulmonary valve, and bifurcation of the branch pulmonary arteries. Obstruction at or below the valve is manifested by a systolic ejection murmur at the left upper sternal border. Distal branch pulmonary artery stenosis radiates this ejection murmur to the axillae and posterior lung fields. An individual patient’s physical examination may vary over time as progressive hypertrophy of the right ventricular outflow increases subvalvar obstruction. Auscultatory findings also may suddenly change with superimposition of reactive dynamic obstruction and virtual occlusion of the right ventricular outflow.
The VSD associated with TOF is a lesion that is seen rather than heard. The typically large defect equalizes both right and left ventricular systolic pressure, and accordingly, no shunt murmur is audible. The defect decompresses the obstructed right ventricle by shunting desaturated blood into the left ventricle and the systemic circulation.
There is considerable anatomic variation with TOF. While many affected patients present with a systolic ejection murmur and cyanosis, some are clinically acyanotic. In such cases, a fortuitous physiologic balance exists between the large VSD and the degree of right ventricular outflow obstruction. The potential for excessive pulmonary blood flow with left-to-right shunting across a large VSD is moderated by right ventricular outflow tract obstruction. These infants may have an uneventful course until elective surgical intervention is performed to close the VSD and relieve the outflow obstruction. Until surgical correction is performed, however, these children remain at risk for hypercyanotic episodes due to acute increase in dynamic obstruction of the right ventricular outflow.
One of the most clinically challenging variations of TOF is the neonate who also has atresia of the pulmonary valve. This infant may be minimally cyanotic at birth as a result of persistent shunting across the patent ductus arteriosus (PDA) or the presence of systemic-to-pulmonary artery collaterals that preserve pulmonary blood flow.
When pulmonary blood flow is totally ductal dependent, the infant may become rapidly and profoundly cyanotic with spontaneous closure of the ductus arteriosus. These infants require emergency intervention with initiation of prostaglandin E-1 therapy and surgical placement of a systemic-to-pulmonary artery shunt.
Those infants with TOF and pulmonary atresia whose pulmonary blood flow depends on multiple systemic-to-pulmonary artery collaterals may not present clinically for several weeks following discharge home. These infants often have complex pulmonary artery anatomy, with marked hypoplasia or even absent branch segments.
Left Heart Obstructive Anomalies That are Ductal Dependent
In utero, the ductus arteriosus effectively bypasses anomalies of the great vessels (Fig. 37-1), AV and semilunar valves, and hypoplasia of the ventricles. Congenital cardiovascular anomalies of the left heart that are well palliated in the fetus and newborn by the PDA and placental circulation may present acutely and precipitously in the newborn period following spontaneous closure of the ductus arteriosus. Following birth, patency of the ductus arteriosus can transiently preserve systemic or pulmonary circulation. In neonates with critical aortic stenosis or coarctation of the aorta, closure of the ductus in the first 48 to 96 hours of life is followed by progressive metabolic acidosis and myocardial dysfunction. The challenge is to identify affected infants before clinical deterioration alters the opportunity for successful surgical management.
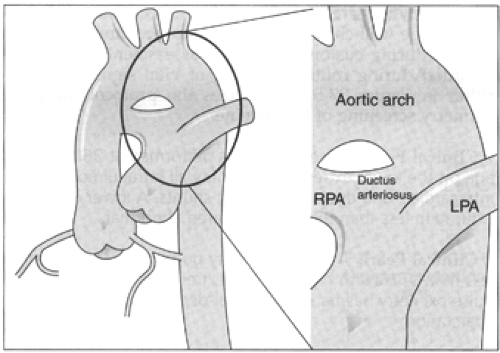 Figure 37-1 Normal ascending aorta, transverse aortic arch, and descending aorta with large ductus arteriosus bridging the main pulmonary artery. The diameter of the normal ductus arteriosus in the fetus and newborn, prior to closure, approximates that of the transverse aortic arch. |
Meeting the challenge of early diagnosis of ductal-dependent cardiovascular anomalies requires more than a clinician’s high index of suspicion. The neonate with clinically occult coarctation of the juxtaductal aorta is an example of how a large PDA can obscure clinical acumen (Fig. 37-2). Right-to-left shunting across a neonate’s unrestrictive PDA provides effective systemic
blood flow distal to the severest of aortic arch anomalies. Femoral pulses are preserved, and the discrepancy in saturation between the upper and lower extremities may not be clinically apparent. Subtle respiratory changes due to progressive left ventricular failure may not be appreciated until spontaneous closure of the PDA compromises peripheral perfusion. Metabolic acidosis then results. A similar clinical pattern occurs with hypoplasia of the left heart where right-to-left shunting across the ductus arteriosus is necessary to palliate aortic or mitral atresia (see Fig. 37-2).
blood flow distal to the severest of aortic arch anomalies. Femoral pulses are preserved, and the discrepancy in saturation between the upper and lower extremities may not be clinically apparent. Subtle respiratory changes due to progressive left ventricular failure may not be appreciated until spontaneous closure of the PDA compromises peripheral perfusion. Metabolic acidosis then results. A similar clinical pattern occurs with hypoplasia of the left heart where right-to-left shunting across the ductus arteriosus is necessary to palliate aortic or mitral atresia (see Fig. 37-2).
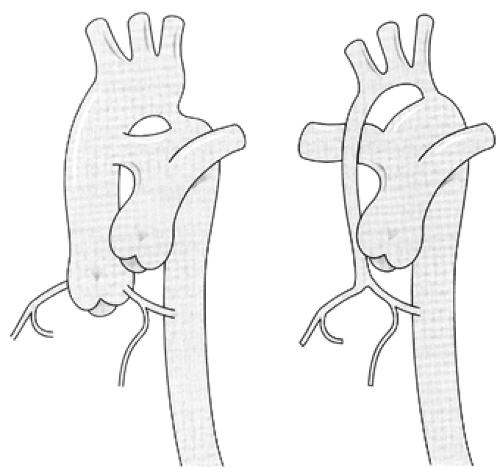 Figure 37-2 (Left) Simple coarctation of the juxtaductal aorta with unrestrictive ductus arteriosus confluent with proximal descending thoracic aorta. (Right) Aortic valve atresia with hypoplastic proximal ascending aorta originating at confluence of right and left main coronary arteries and continuing as hypoplastic transverse aortic arch. The confluence of an unrestrictive ductus arteriosus preserves antegrade blood flow to the descending aorta and retrograde flow to the transverse aortic arch, ascending thoracic aorta and coronary arteries. |
Identification of congenital cardiovascular anomalies when patency of the PDA preserves systemic or pulmonary (Fig. 37-3) blood flow is a challenge for the pediatric clinician. It is critical to identify ductal-dependent lesions so that prostaglandin E-1 therapy can be initiated to keep the ductus arteriosus patent and preserve pulmonary or systemic blood flow.
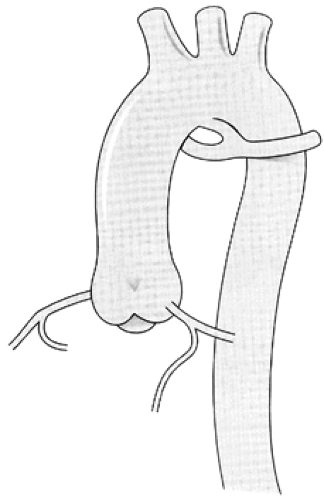 Figure 37-3 Dilated proximal ascending aorta continuous with transverse aortic arch from which a “reverse” ductus arteriosus communicates with hypoplastic, confluent branch pulmonary arteries in a neonate with atresia of the main pulmonary artery and pulmonary valve. The reverse ductus, so called because of its more anterior origin from the inferior aspect of the transverse aortic arch, preserves antegrade branch pulmonary artery blood flow. |
Ductal-dependent anomalies may not be apparent during initial physical examination in the newborn nursery.
The infant’s subsequent presentation following spontaneous closure of the PDA is heralded by either significant cyanosis or, in the case of left-sided obstruction, profound metabolic acidosis and shock. Fetal echocardiography allows antenatal diagnosis of most ductal-dependent anomalies. However, cost and availability limit its application as a universal screening procedure.
Diagnostic Studies
It is obvious that a small but significant number of newborns with either cyanotic congenital heart anomalies or those with defects that depend on the ductus arteriosus to maintain critical systemic or pulmonary blood flow will be missed by even the most careful of physical examinations. Pulse oximetry, however, can identify ductal-dependent lesions and systemic oxygen desaturation in neonates with right-to-left intrapulmonary or intracardiac shunts.
Most clinicians are familiar with the partial pressure of oxygen (pO2) reported on arterial blood gas samples. This is a measure of the oxygen concentration dissolved in plasma regardless of hemoglobin binding. Arterial oxygen saturation,
however, is a measure of the percent of oxygen bound to hemoglobin. Oxygen capacity is the maximum predicted volume of oxygen that can be bound to hemoglobin (1.34 mL oxygen per gram of hemoglobin) in a sample of blood. The oxygen content is the measured amount of oxygen actually bound to hemoglobin in blood from a specific vessel (eg, the aorta). The oxygen saturation, expressed as a percent is the simple fraction relating oxygen content and capacity:
however, is a measure of the percent of oxygen bound to hemoglobin. Oxygen capacity is the maximum predicted volume of oxygen that can be bound to hemoglobin (1.34 mL oxygen per gram of hemoglobin) in a sample of blood. The oxygen content is the measured amount of oxygen actually bound to hemoglobin in blood from a specific vessel (eg, the aorta). The oxygen saturation, expressed as a percent is the simple fraction relating oxygen content and capacity:
Pulse oximetry offers a repetitive, noninvasive measure of systemic oxygen saturation using the distinctive light absorption properties of oxygenated and deoxygenated hemoglobin in pulsating tissue (Poets & Martin, 1996). Sampling can be performed from the upper and lower extremities as well as the nares or ear lobes.
In the normal neonate, virtually all arterial hemoglobin is bound to oxygen, and the systemic arterial (aortic) saturation is greater than 95%. Right-to-left shunting, either due to pulmonary parenchymal disease or intracardiac/extracardiac shunting reduces the aortic oxygen saturation. If the right-to-left shunt occurs in the lungs or within the heart, then the systemic oxygen saturation is decreased no matter where the pulse oximetry probe is applied to the infant. If, however, right-to-left shunting occurs across the PDA, then the pulse oximetry oxygen saturations in the upper extremities will be higher than those recorded in the lower extremities (Fig. 37-4). Along with other surveillance protocols, pulse oximetry screening is an efficient technology applicable to large well child nurseries. The procedure can be performed during customary nursing assessment with results recorded during routine charting of vital signs. The algorithm in Figure 37-5 summarizes the protocol for pulse oximetry screening of the neonate.
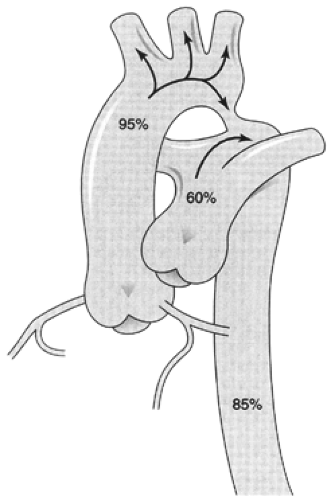 Figure 37-4 Illustration of oxygen saturations in the ascending aorta, main pulmonary artery, and descending aorta associated with right-to-left shunting across an unrestrictive ductus arteriosus with critical juxtaductal coarctation of the aorta. Simultaneous pulse oximetry of the right upper and right or left lower digits would reveal an oxygen saturation gradient between the upper extremities (95%) (perfused by subclavian arteries arising proximal to the right-to-left ductus arteriosus shunt) and the more distal lower extremities (85%) perfused by the descending aorta. |
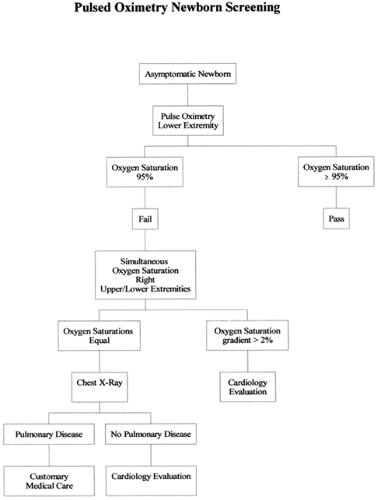 Figure 37-5 Algorithm used at the Schneider Children’s Hospital for universal newborn pulse oximetry screening to identify cyanotic and ductal-dependent congenital heart disease. |
• Clinical Pearl
Pulse oximetry is performed at 36 hours of age on the lower extremity to identify all intrapulmonary, intracardiac, and ductal-dependent shunts. A lower extremity saturation less than 95% is considered abnormal.
• Clinical Pearl
A lower extremity pulse oximetry saturation less than 95% with higher upper extremity saturations is the pulse oximetry hallmark of a ductal-dependent aortic coarctation.
The neonate with critical coarctation of the aorta will have a saturation gradient between the upper and lower extremities due to right-to-left ductal shunting. However, the upper extremity saturation may not be normal if the infant has pulmonary venous congestion that interferes with normal gas exchange and lowers the saturation of pulmonary venous blood.
• Clinical Pearl
In neonates with hypoplastic left heart complex and aortic atresia, global systemic desaturation is present with no saturation gradient between the upper and lower extremities.
The absence of a pulse oximetry gradient between the upper and lower extremities and the globally reduced systemic saturation reflect common mixing of pulmonary venous and systemic venous blood in the atria in the presence of mitral and aortic atresia or single ventricle.
The utility of pulse oximetry extends beyond screening in the management of congenital heart disease. It also provides effective surveillance following interventions to stabilize neonates with ductal-dependent circulation. Prior to medical intervention, the acidotic neonate with critical coarctation and spontaneous closure of the PDA will have no saturation gradient between the upper and lower extremities. In the absence of pulsatile flow due to the proximal coarctation, no saturation in the lower extremity can be documented. Following initiation of prostaglandin E-1 therapy, pulse oximetry of the lower extremity provides evidence of pulsatile flow as ductal patency is restored and a systemic oxygen saturation gradient is established.
Right-to-left shunting across the PDA and its surveillance with pulse oximetry is not restricted to neonates with complex congenital heart disease. A common application of this clinical tool is in newborns with persistence of fetal-type circulation (Walsh-Sukys et al., 2000). Neonates with persistent elevation of pulmonary artery resistance and pressure following meconium aspiration or birth asphyxia often demonstrate right-to-left shunting across both the interatrial septum and PDA. Medical therapies for management of this problem (Davidson et al., 1998) are directed to increase effective pulmonary blood flow while the infant recovers from related pulmonary parenchymal injury. Reduction in pulmonary artery pressure and resistance, as oxygenation and gas exchange improve, can be monitored with surveillance of the oxygen saturation gradient between the upper and lower extremities. As pulmonary artery pressure and resistance decrease, the oxygen saturation gradient between the upper and lower extremities will fall until right-to-left shunting across the PDA ceases.
THE INNOCENT MURMUR
Evaluation of the preschool child with a nonradiating, vibratory systolic ejection murmur at the left mid and upper sternal borders remains a common problem for the primary care practitioner (Sapin, 1997) and a debatable cause for pediatric cardiology referral. This auscultatory finding in an otherwise normal child at a well child examination, or the child with normal past medical history presenting with an intercurrent febrile illness, often escalates beyond its clinical relevance due to parental concern.
The term innocent murmur refers to an auscultatory finding heard in the majority of children at some time in their lives. Many clinicians prefer to label these murmurs “innocent” rather than “functional,” because the former is a much more reassuring term to parents and patients. The critical issue for the primary care provider is to be able to distinguish these murmurs from those caused by true organic heart problems.
History and Physical Examination
• Clinical Pearl
The innocent murmur’s quality and timing, the changing intensity from supine to sitting, and the presence of normal splitting of the second heart sound are critical differentiating characteristics.
Quality and Timing
The physical examination of the normal infant, toddler, and young child is often punctuated by the discovery of “functional” murmurs. They are ejection type and have a vibratory or musical quality.
These murmurs are always systolic; diastolic murmurs are never innocent. In the majority of toddlers and young children, the left upper/midsternal border “innocent” or vibratory systolic ejection murmur is evidence of accelerated blood flow across the right ventricular outflow tract or central systemic veins. The truncated shape of the right ventricle due to continuity of its capacious tricuspid valve annulus and body with a conical shaped tapering outflow accelerates blood flow. The change in velocity of blood flow through the normal right ventricle is similar to that of water in a stream whose channel narrows. The sound of water accelerating as the stream’s banks converge parallels the functional murmur, audible at the left upper sternal border of the heart, as blood accelerates across the normal right ventricular outflow tract.
If the volume of blood returning to the right heart is increased, either by febrile illness, anemia, or posture, the intensity of the murmur increases much as the sound of the stream does with runoff following a rainfall. This explains the frequent discovery of a “new” or “never heard before” murmur during the evaluation of a routine febrile illness.
Change from Supine to Sitting
• Clinical Pearl
Distinguishing the normal, typically grade 1 to 2/6, vibratory, systolic ejection flow murmur from that of a cardiovascular anomaly begins with altering the patient’s posture. Arising from a supine to an upright posture decreases systemic venous return to the right heart, reducing the intensity and possibly silencing the systolic ejection murmur.
While murmurs secondary to structural cardiovascular anomalies can be influenced by changes in systemic venous return to the heart, simple postural changes usually have a minimal effect on the intensity of organic murmurs.
• Clinical Pearl
Murmurs related to structural cardiovascular anomalies, particularly the systolic ejection murmur of dynamic left ventricular outflow tract obstruction or the insufficiency murmur of mitral valve prolapse, will often increase in intensity with decreased venous return to the heart (supine to upright).
Postural changes in intensity help identify most murmurs of “functional origin.” Interpretation of the response to such maneuvers, however, may be confusing. While upright posture decreases venous return from the inferior vena cava, it accelerates superior vena cava as well as innominate, subclavian, and internal jugular venous blood flow. This acceleration in blood flow often results in a continuous, infraclavicular venous hum that may simulate a PDA in the toddler or young child. Discriminating the continuous murmur of the venous hum from that of a PDA is straightforward. The venous hum continuous murmur is exquisitely sensitive to maneuvers reducing superior venous blood flow velocity. The transition from upright to supine posture, contralateral rotation of the head, or gentle supraclavicular compression eliminates the venous hum murmur but does not influence the continuous murmur of the PDA.
Physiologic Splitting of the Second Heart Sound
• Clinical Pearl
The single first and the softer, variably split second heart sound (S2) are the auscultatory hallmarks of the normal heart.
Being able to identify variability or physiologic splitting of S2 is often a challenge, especially in younger children. Concentrating on that particular phase of the cardiac cycle requires patience. In older cooperative children, asking for deep breathing in and out and holding the breath may make variable splitting more apparent.
Hearing variability in the splitting of S2 commonly differentiates between the ejection-type flow murmur of an innocent murmur, an ASD, and those murmurs caused by right sided outflow tract obstruction. All of these murmurs sound the same in that they are typical ejection type murmurs; S2 splitting differentiates between the three. Innocent murmurs have variable splitting.
The murmur of an ASD is caused by relative pulmonic stenosis. This is due to increased blood volume across a normal pulmonic valve due to inter-atrial left-to-right shunting, and it sounds like a typical pulmonic ejection-type murmur (the sound of the murmur is not caused by flow across the ASD). Because of the increased flow, closure of the pulmonic valve lags behind aortic valve closure, resulting in a fixed and widely (nonvariable) split S2. With the murmur of pulmonic stenosis, it is typically difficult to identify any normal splitting of S2.
Diagnostic Criteria
The experienced provider will be able to differentiate innocent (functional) murmurs from their organic counterparts by the three auscultatory characteristics described previously. If all three criteria are not met or if there is clinical uncertainty, then further evaluation is recommended. Depending on local circumstances, this may involve two-dimensional echocardiography, referral to a pediatric cardiologist, or both.
Functional murmurs are encountered in the newborn and younger infant. It is imperative, however, to remain vigilant for subtle clinical evidence of congenital heart disease. A short systolic ejection murmur with no diastolic component and localized at the left upper sternal border may accompany normal closure of the ductus arteriosus in the first few days of life. A restrictive, pinhole sized apical or midmuscular VSD may produce a short, regurgitant murmur at the left lower sternal border shortly after birth. Peripheral pulmonic stenosis, the normal perinatal discrepancy between the main and branch pulmonary arteries’ diameters during the first few weeks of life, accelerates blood flow, resulting in a systolic ejection murmur audible at the left upper sternal border and radiating to the axillae and interscapular areas.
Management
Once the provider establishes the diagnosis of an innocent murmur, he or she must be clear and precise in explaining to both parent and patient that the murmur is truly a normal variant. A good explanation is that the sound is caused by blood rushing through a healthy, young, elastic, and normal heart. The provider must emphasize that there is no need for any further testing, referral to a cardiologist, limitation of activity, or endocarditis prophylaxis.
The diagnosis should be clearly documented in the health record, however. Any future intercurrent illness, particularly with fever, will no doubt reveal a louder but also completely innocent murmur. If this evaluation is performed by someone other than the usual provider, having the parent or patient fully informed of the previous finding, as well as having it documented clearly in the record, will alleviate undue anxiety and eliminate the need for further unnecessary testing.
CHEST PAIN
Chest pain is a common chief complaint encountered in the primary care practice office. Nontraumatic chest pain is rarely associated with structural cardiovascular disease in this population. Most chest discomfort in older children and adolescents is secondary to transient musculoskeletal or esophageal dysfunction.
However, certain organic problems can occur in children and adolescents that do require prompt assessment and intervention. They include pericardial inflammation, myocardial ischemia secondary to accelerated atrial or ventricular arrhythmias, pulmonary parenchymal or pleural disease, and spontaneous vascular injury. The usually aggressive diagnostic and therapeutic interventions applied to the symptomatic adult patient with chest pain must be modified in the evaluation and management of the more benign etiologies of chest discomfort in children.
Unlike the adult describing crushing anginal symptoms of myocardial ischemia, the child or adolescent frequently has difficulty characterizing the symptomatology that prompted medical evaluation. The practitioner is often confronted with a report of nonspecific, transient, anterior chest discomfort that is vague in quality, poorly localized, and variably associated with activity or posture. While such ill-defined chest pain in the pediatric population is often functional, there is a subset of neonates, children, and adolescents with organic chest discomfort that may be obscured by the patient’s communicative skills.
The precordial discomfort of sustained supraventricular tachycardia with ventricular pre-excitation of Wolf-Parkinson-White in a young child, the aching sensation of pericardial inflammation in an adolescent awakening in the middle of the night, or colic-like symptoms secondary to myocardial ischemia of coronary artery anomalies in an infant require timely diagnosis and intervention. Discrimination between the chest pain of self-limiting, benign musculoskeletal or gastroenteric dysfunction in an otherwise well pediatric patient and that due to far less common, but potentially life-threatening, organic disease is a clinical challenge.
History and Physical Examination
Management of chest pain is guided by pertinent findings in the patient’s medical and family history and description of symptoms in terms of their duration, location, quality, and the circumstances provoking discomfort. Figure 37-6 illustrates clinical cues for assessment of chest pain in this population.
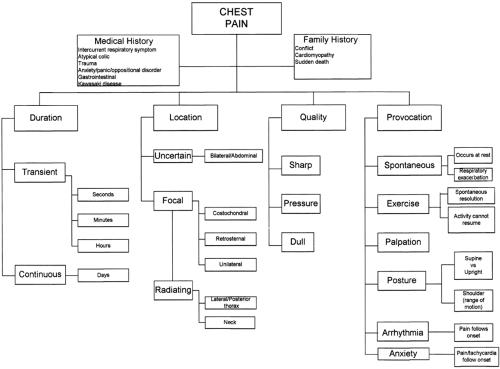 Figure 37-6 Algorithm for assessment of chest pain in the pediatric population. There is considerable overlap in clinical expression of functional and organic causes of chest pain. Their discrimination, however, is facilitated by a systematic approach that begins with the patient’s medical and family history, followed by determination of symptom duration, localization, quality, and inciting or provocative factors. The majority of benign chest pain referred for pediatric cardiology assessment includes a noncontributory medical history with no organic family history. The duration of pain is reported as seconds, the location is vague and referred primarily to anterior chest wall bilaterally, and the quality is sharp or knife-like and exacerbated by deep respiration. It resolves spontaneously in minutes with voluntary resumption of full activity. |
History
Antecedent viral illness is commonplace during the winter and spring months. Temporal relationship to symptoms help pinpoint the prodrome, which precedes pericardial or pleural disease. Marfan syndrome in first- or second-degree relatives of a phenotypically suggestive, tall adolescent presenting with a spontaneous pneumothorax should direct the clinician’s attention to connective tissue disease, especially when scoliosis, pectus excavatum, or abdominal wall hernias have been treated or noted in the past. Such patients may present with acute chest pain radiating to the neck or back secondary to spontaneous injury of an aortic aneurysm (Groenink et al., 1999). Past medical history of Kawasaki syndrome or an atypical febrile illness associated with a perineal rash, edema of the hands and feet, or mucoconjunctivitis warrants investigation of coronary artery anatomy. A history of intractable colic and poor weight gain in the young infant may be the only manifestation of abnormal coronary artery (anomalous origin of the left coronary artery from the pulmonary circulation). The child or adolescent reporting a tapping sensation in the chest or vague chest discomfort with irregular heartbeats may be experiencing tachyarrhythmias related to atrial or ventricular ectopy.
Discrimination between benign functional and organic chest pain can often be accomplished with review of the symptoms’ duration, location and quality of the discomfort, and circumstances provoking the complaint.
Duration of Symptoms
Patients with benign, fleeting chest discomfort of musculoskeletal or transient gastrointestinal etiology find it difficult to be precise about the onset of symptoms that are fleeting in quality and rarely interrupt their activity. In contrast, those with organic chest pain can often pinpoint the onset of symptoms and are emphatic about its chronicity.
• Clinical Pearl
The more precise and specific the description of the chest pain is, the more likely the etiology is truly organic. For example, patients with inflammatory pain, such as pericarditis, report how the persistent discomfort interferes with sleep throughout the night.
The timelines of chest pain in the pediatric population vary according to etiology. Pain due to self-limiting musculoskeletal or gastrointestinal etiologies is fleeting, lasting only seconds. A spontaneous pneumothorax results in acute penetrating pain that wanes. Myocardial ischemia results in minutes of provocable anginal discomfort. Pleuropericardial inflammation and costochondritis result in an incessant ache.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


