Hearing Impairment and Disorders
Stella C. Laufer Turk MS, CCC-A, FAAA
Anne C. Balant PhD, CCC-A
INTRODUCTION
Communication is the most fundamental component of human interaction and learning. Sound production, perception, and understanding are prerequisite to spoken language learning, and, ultimately the attainment of higher level cognitive skills. The healthy neonate is prepared to begin the process of language development and can perceive sounds at birth, although responses such as the ability to localize to the direction of a sound source continue to mature during infancy. Assessment of hearing may be performed within hours after birth through behavioral observation by a trained examiner and by tests such as the auditory brainstem response or otoacoustic emissions.
Without intervention, hearing impairment has a calamitous effect on the speech and language development of a child. Impairment may also cause significant deficits in educational and psychosocial development. Even minimal, unilateral, and transient hearing loss from otitis media has been shown to have a detrimental impact (Bess, Dodd-Murphy, & Parker, 1998). Children who receive intervention for hearing loss within the first 6 months of life have significantly better language outcomes and improved overall development in a number of areas, compared with those who receive later intervention (Yoshinaga-Itano, 1998; Yoshinaga-Itano & Apuzzo, 1998).
Diagnosis and intervention must take place during the first year of life, ideally within the first 6 months. At present, the age of identification of hearing loss in the United States still averages 12 to 25 months, with an additional delay of up to 1 year prior to intervention. These averages are far from the U.S. Department of Health and Human Services’ Healthy People 2010 goal of increasing “to 100 percent the proportion of newborns who are screened for hearing loss by 1 month of age, have diagnostic follow-up by 3 months and are enrolled in appropriate intervention services by 6 months” (1999, section 12, objective 33). Delays in identification and intervention have been attributed to the following three factors:
Universal infant hearing screening is not yet widespread.
Many parents are unaware of the indicators of hearing loss.
Primary care providers often respond to parental concerns with a “wait and see” attitude instead of a referral for audiologic evaluation (U.S. Department of Health and Human Services, 1999).
Established screening programs have documented success in reducing the age of identification and intervention for hearing loss, and their performance improves with time. For example, the Rhode Island Hearing Assessment Program decreased its initial mean ages of confirmation (8.7 months) and intervention (13.3 months) to 3.5 months and 5.7 months respectively from 1993 to 1996 (Vohr, Carty, Moore, & Letourneau, 1998). Universal infant hearing screening programs, such as the Rhode Island initiative, are highly sensitive, specific, and cost effective.
• Clinical Pearl
Problems associated with delay could be reduced through more widespread implementation of universal infant hearing screening.
Infant hearing screening is inexpensive compared with other forms of disease screening, with a cost ranging from about $10.00 to $30.00 per infant screened or about $5000.00 to $10,000.00 per hearing loss identified (Maxon, White, Behrens, & Vohr, 1995; Mehl & Thomson, 1998). The cost of screening plus intervention for those with hearing loss has been shown to compare favorably with the cost of special education and language services that would otherwise be required (Mehl & Thomson, 1998). Useful guidelines for infant hearing screening programs have been published by a task force of the American Academy of Pediatrics (Erenberg, Lemons, Sia, Trunkel, & Ziring, 1999). A model of a typical hospital-based infant hearing screening program can be found in Appendix 53-1.
Even when infants receive hospital-based hearing screening, there is always the possibility of a later onset or progressive hearing impairment. For these infants, parental concern is often the chief means of identification. Typically, such concerns are initially addressed with the child’s primary care provider. Therefore, the primary care provider forms a crucial link between children who have or are at risk for hearing loss and the wide range of services available to meet their needs. One of the objectives of the draft of Healthy People 2010 guidelines (1999) is to “increase the proportion of primary care providers who routinely refer or screen infants and children for impairments of vision, hearing, speech, and language… as part of well-child care” (U.S. Department of Health and Human Services, Section 12, objective 38). Early identification of hearing loss, frequent monitoring, appropriate medical and rehabilitative intervention, and realistic parental counseling continue to be the best means to reduce the devastating impact of hearing loss.
ANATOMY, PHYSIOLOGY, AND PATHOLOGY
When an airborne sound wave enters the ear canal, it is amplified, filtered, and converted by the intricate structures of the auditory system from acoustic to mechanical to electrochemical energy and ultimately to neural impulses. These neural impulses are organized by their timing and place within the auditory system, from cochlea to auditory cortex. Understanding the anatomy and physiology of the auditory system is essential to understanding how its different sections are affected by pathologies.
The system is often divided into the peripheral (outer, middle, and inner ear) and central auditory systems. To facilitate the understanding of the interrelationship between anatomy, physiology, and pathology, the divisions that are used here are related to possible sites of lesions, including the following:
Conductive system (outer and middle ears)
Sensorineural system (cochlea including the distal ends of the cochlear nerve fibers)
Central auditory pathways (remainder of cranial nerve VIII through the auditory cortex)
Conductive System
The conductive system transfers the acoustic signal to the inner ear and protects the ear’s more delicate structures. Pathology, owing to obstructions or improperly functioning structures, may reduce the sound available to the normally functioning inner ear. The loss may range from mild to moderate-severe, and it may be temporary or permanent. Most conductive hearing losses are treatable with medication or surgery. Figure 53-1 presents the peripheral auditory system.
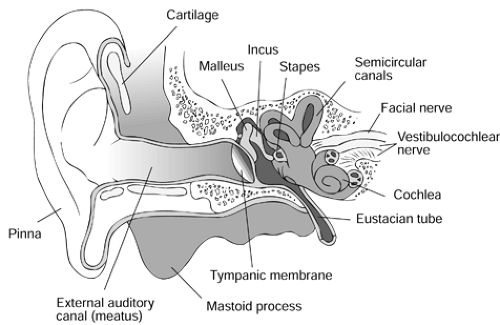 Figure 53-1 Peripheral auditory system. |
Outer Ear
The auricle, or pinna, and external auditory meatus comprise the outer ear. The pinna has minimal effect on hearing sensitivity, but its irregular shape aids in sound source localization (ie, directional hearing). The shape and length of the meatus provide a resonant effect by amplifying sound in the range of 2000 to 5000 Hz in adults. These are important frequencies for speech perception. Higher-frequency resonances are observed in infants and children. The ear canal directs sound waves to the tympanic membrane (TM), or eardrum.
Disorders of the outer ear include the following (conditions marked with an asterisk are associated with hearing impairment):
Congenital structural anomalies* (microtia, aplasia, aural stenosis)
Impacted cerumen*
Foreign bodies
Growths and tumors
Otitis externa
Necrotizing external otitis
Herpes zoster oticus* (associated with sensorineural hearing loss, vertigo, and facial palsy)
Middle Ear
The middle ear, or tympanic cavity, is an air-filled cavity medial to the external auditory meatus. It includes the TM, ossicular chain, middle ear muscles, eustachian tube, and the oval and round windows. The healthy TM appears pearly gray, translucent, and concave through the otoscope. The cone of light, a triangular reflection of light from the otoscope, is usually evident. At birth, the TM is obliquely angled so that it almost lies on the floor of the canal. As the canal grows and lengthens, the TM becomes more upright and hence more visible on otoscopic examination.
The ossicular chain is made up of the three smallest bones in the human body: the malleus, incus, and stapes. They are fully developed at birth. The structures of the middle ear help to overcome the difference in mechanical impedance between the air in the ear canal and the fluids of the cochlea by approximately 30 decibels (dB). The eustachian tube opens into the anterior wall of the middle ear at one end and the nasopharynx at the other, allowing equalization of the middle ear with ambient air pressure and drainage of middle ear secretions into the nasopharynx. In children, the tube is shorter, wider, more horizontal, and more flexible than in adults. This leads to a greater susceptibility to spread of upper respiratory infections. Abnormal patency, intrinsic closure, and extrinsic closure of the tube can lead to atelectasis, negative middle ear pressure, and effusion.
The tensor tympani and the stapedius muscles are the smallest striated muscles in the body. They contract reflexively
and stiffen the ossicular chain to protect the inner ear against some types of high-level acoustic signals. This acoustic reflex can be elicited by an acoustic signal 80 to 90 dB above an individual’s auditory threshold. Because the onset of the acoustic reflex is not immediate, it cannot protect the ear against explosive sounds. The audiologist tests the integrity of the auditory nerve, cranial nerve VIII (afferent supply), and the facial nerve, cranial nerve VII (efferent supply), by eliciting an acoustic reflex as part of an acoustic immittance test battery (American Speech-Language Hearing Association, 1990).
and stiffen the ossicular chain to protect the inner ear against some types of high-level acoustic signals. This acoustic reflex can be elicited by an acoustic signal 80 to 90 dB above an individual’s auditory threshold. Because the onset of the acoustic reflex is not immediate, it cannot protect the ear against explosive sounds. The audiologist tests the integrity of the auditory nerve, cranial nerve VIII (afferent supply), and the facial nerve, cranial nerve VII (efferent supply), by eliciting an acoustic reflex as part of an acoustic immittance test battery (American Speech-Language Hearing Association, 1990).
Disorders of the middle ear include the following (conditions marked with an asterisk are associated with hearing impairment):
Congenital structural anomalies*
Acoustic trauma and barotrauma*
TM perforation*
Eustachian tube dysfunction
Ossicular discontinuity or fixation*
Glomus tympanicum and glomus jugular tumors*
Otitis media*
Cholesteatoma*
Sensorineural System
The sensorineural system consists of the inner ear, or cochlea, and the distal ends of the cochlear nerve fibers. In some types of hearing loss (eg, due to aging), both the cochlear and the cochlea nerve are affected, so a cochlear hearing loss is referred to collectively as a sensorineural hearing loss. This is sometimes mistakenly termed a nerve loss. Sensorineural hearing loss typically reduces the overall dynamic range of the auditory system, in that soft sounds are not perceived well but loud sounds are perceived almost normally. The loss may be stable or progressive, but it usually is irreversible.
The sensory organ for hearing is the organ of Corti. It is housed within a snail-shaped continuation of the osseous labyrinth called the cochlea. The cochlea is 35 mm in length, coiling approximately 2½ times around a bony core, the modiolus. The outer hair cells actively modify the properties of the cochlea, increasing its sensitivity and its ability to resolve individual frequencies of sound and generating otoacoustic emissions. The inner hair cells deliver auditory information in an organized fashion to the fibers of cranial nerve VIII. Damage to hair cells or associated structures leads to sensorineural hearing loss.
Disorders associated with sensorineural hearing impairment include the following:
Congenital inner ear anomalies or dysplasias
Perilymphatic fistulas
Trauma
Noise-induced hearing loss
Ototoxicity-induced hearing loss
Congenital perinatal infections
Other etiologies for hearing loss are discussed in the section History and Physical Examination.
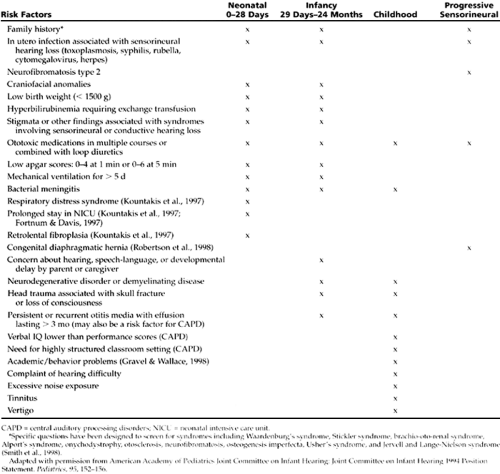
Children with congenital diaphragmatic hernia who present with severe neonatal respiratory failure are at high risk of developing sensorineural hearing loss within the first 2 to 5 years of life (Robertson, Cheung, Haluschak, Elliot, & Leonard, 1998). Infants and children with this or any of the other risk factors for progressive hearing loss listed in Table 53-1 require periodic audiologic monitoring.
Infants and children are more vulnerable to the effects of hazardous noise at lower levels than are adults. Some commercially available toys may produce hazardous noise levels if held too close to the ear.
Children and teens must be monitored to keep volume down on televisions, personal stereo headsets, and car stereo systems. Use of hearing protection is essential for children or teens who are exposed to firearms, snowmobiles, power tools, and other sources of potentially hazardous noise.
Central Auditory Pathways
The central auditory nervous system consists of complex, interwoven neural pathways extending from the cochlea through the brainstem and midbrain to the auditory areas of the cortex. Specific sites along these pathways may be affected by retrocochlear disorders, such as neurofibromatosis. In contrast, central auditory processing disorders (CAPD) in children are not usually linked to an identifiable lesion in these pathways. Central auditory processing is defined as “what we do with what we hear.” Hence, CAPD is a disorder in the mechanisms or processes that are responsible for the following (adapted from ASHA, 1996):
Sound localization and lateralization
Auditory discrimination and pattern recognition
Temporal aspects of audition, including temporal resolution, masking, integration, and ordering
Auditory performance decrements with competing or degraded acoustic signals
Diagnosis of CAPD is based on history and performance on diagnostic tests.
• Clinical Pearl
CAPD should be considered when a child is having academic difficulties and hearing loss or developmental disabilities have been ruled out. Referral to a speech-language pathologist and audiologist is indicated. Children with CAPD may be effectively managed with various strategies, including assistive devices recommended by an audiologist. These devices improve intelligibility of speech in the classroom.
Disorders of the central auditory pathways that can affect hearing include the following (conditions marked with an asterisk are associated with hearing impairment):
Retrocochlear lesions* (acoustic neuromas [eg, neurofibromatosis type 2])
Hydrocephalus*
Associated conditions include the following:
Chronic otitis media with conductive hearing loss*
Attention deficit disorder/attention deficit-hyperactivity disorder
Language learning disability
Children with a history of recurrent middle ear pathology who demonstrate speech and language deficits or other educational delays should not be expected to recover these skills spontaneously when hearing returns to the normal range.
• Clinical Pearl
Refer any child with recurrent otitis media for an audiologic evaluation. A clear picture of the degree of communication handicap is extremely helpful in documenting the need for additional referrals, such as otolaryngology, speech-language pathology, and educational evaluation.
EPIDEMIOLOGY
The reported prevalence rates of peripheral hearing loss among children are quite variable. These values depend both on age and on the type and severity of the hearing loss (ie, unilateral versus bilateral, conductive versus sensorineural).
Newborns and Infants
The prevalence rates of peripheral hearing loss in newborns and infants include the following:
1 to 2 per 1000 have a permanent bilateral hearing loss (Vohr et al., 1998; Fortnum & Davis, 1997).
About 6 per 1000 infants exhibit all types of losses, including unilateral and conductive.
Among infants who are “at risk,” 30 to 50 per 1000 have such a loss (Kittrell & Arjmand, 1997).
A higher incidence of hearing loss may be operant among male children of African American heritage (Van Naarden, Decoufle, & Caldwell, 1999). The age of diagnosis
has been reported to be later in non-Caucasian than Caucasian children, regardless of socioeconomic status (Kittrell & Arjmand, 1997; Kountakis, Psifidas, Chang, & Stiernberg, 1997).
About one half of all congenital hearing impairment is associated with the neonatal risk factors originally identified by the Joint Committee on Infant Hearing (Mehl & Thomson, 1998; Yoshinaga-Itano & Apuzzo, 1998). These and additional neonatal risk factors recently mentioned in the literature are listed in Table 53-1.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


