Healthy Growth and Development of the School-Age Child
Andrea Berne RN, CPNP, MPH
Ellen Flynn RN, CPNP
INTRODUCTION
The school-age period (5–12 years of age) is a time of relatively slow but steady growth. It is a time of quiescence during which the primary care provider can rely on both the parent and child to give a history that directs the focus of the encounter. Excluding dentition and pubertal change, organs are developed and fully functioning. Major illness is not expected. Problems usually involve routine infection, known allergy, sports, and other injuries.
Many school-age children present with complaints of benign aches and pains of various body systems (eg, stomach ache, headache, and leg pain). The school-age child with a previously diagnosed chronic illness needs support to begin participating in the management of that illness. School entry and adjustment bring their own physical, developmental, psychological, and social challenges. During this period, learning difficulties, attention problems, and affective disorders surface.
The school-age child is on an early path toward independence. Successful academic achievement and acceptance from peers help in the development of initiative, competence, and confidence. Because school becomes the most important parameter of the child’s cognitive development, providers must support the family with this transition.
GROWTH AND DEVELOPMENT
Physical Development
School-age children grow at a slow pace until they hit their “growth spurt.” Expected growth is 2 in and 5 to 7 lb per year for both males and females. These parameters are particularly important in the identification of obesity for which today’s school-age children are at high risk. In terms of stature, genetics play a role in normal variations, which may appear below the fifth or above the 95th percentile on standard growth charts. Abnormal etiologies may exist and include chronic illness, endocrine abnormalities, and neglect or abuse. The beginning of rapid adolescent growth for girls can be as early as 9 years of age and as late as 14 years, 6 months. Boys begin their growth spurt between 10 years, 6 months and 16 years. The median age for girls is 12 years; the median age for boys is 14 years (Bickley, Hoekleman, & Bates, 1999).
• Clinical Pearl
Growth charts should be graphed for height and weight at each visit. Significant crossing of percentiles is almost invariably abnormal in females between the ages of 3 and 10 and in males between the ages of 3 and 12.
Pubertal Development
Pubertal changes may begin in the school-age child. For girls, breast bud development is often the first sign of puberty and can appear as early as 7 years, 5 months and as late as 13 years. Normally, pubic hair follows 6 months later (Algranati, 1998). Each Tanner stage requires approximately 1 year, and menses usually begins sometime during breast Tanner stage IV (see Appendix XX) (Goldblum, 1997).
The first sign of puberty in boys is testicular enlargement and scrotal skin thinning, which can appear as early as 9 years and as late as 13 years, 6 months. The median age of occurrence is 11 years, 6 months. The onset of pubic hair growth occurs between 10 and 15 years. Normally, pubic hair appears 6 months after testicular enlargement begins. Penile enlargement occurs between ages 10 years, 6 months and 14 years, 6 months, 1 year after testicular enlargement (Algranati, 1998).
Motor Skills
Muscle bulk, coordination, and strength continue to develop throughout the school-age years. A 5-year-old child should be able to balance on one foot, walk on tiptoe, and tandem walk on a straight line. A 6-year-old child should be able to skip. An 8-year-old child should be able to hop twice on one foot and then on the other. Examples of appropriate fine motor abilities are the 6-year-old child who ties his or her own shoelaces and the 8-year-old child who performs rapid alternating movements of thumb to each finger of the same hand in succession (Algranati, 1998). Genetics help determine each child’s unique skills and abilities. Normal variations include the clumsy child and the exceptionally athletic child.
Cognitive Development
Previously developed language skills become more fluid, resulting in advanced cognitive functioning in the school-age child. Vocabulary and understanding increase. Grammar and articulation are usually correct. Young school-age children ask many questions, solve simple problems, and use fantasy in their thinking processes. Fantasy thinking generates new fears. Between 6 and 11 years, the child further organizes thought and develops memory. He or she reads and reasons more completely.
Psychosocial Development
For the young school-age child, the family is the primary social group. Grade-school children usually have strong family ties and use their own parents or other adults close to the family as role models (ie, the child dresses up like mom). Relationships with parents and siblings are usually harmonious in younger years, becoming more challenging as
puberty approaches. At this time, conflicts with parents regarding limit setting and expectations often arise. As they get older, school-age children begin to establish their independence, psychologically separate from their parents, and build their own identities. As they separate from parents, peers become increasingly important. Parents must recognize this as normal and allow children to separate.
puberty approaches. At this time, conflicts with parents regarding limit setting and expectations often arise. As they get older, school-age children begin to establish their independence, psychologically separate from their parents, and build their own identities. As they separate from parents, peers become increasingly important. Parents must recognize this as normal and allow children to separate.
The peer group provides an arena for older school-age children to establish independence and test out ideas. Friends are especially important during this time, and children begin to conform to a set of group standards. School-age children assume a sex role and engage energetically in group activities. How they view their competencies within these groups determines motivation, perseverance, and resilience. School-age children begin to incorporate values learned at home, in school, and from peers. The older school-age child begins to let go of fears, focusing more on reality. Approval, recognition, and enthusiasm are the hallmarks of the healthy child during this period. Role models shift to other adults outside the home. Normal variants describe personality differences that exist in children who are thought to be “different” but still function acceptably. Normal variants include shy, cautious, or contentious children. Parents need to seek help when a child fails to succeed at the tasks expected for his or her age because these personality differences are interfering with achievement.
HISTORY AND PHYSICAL EXAMINATION
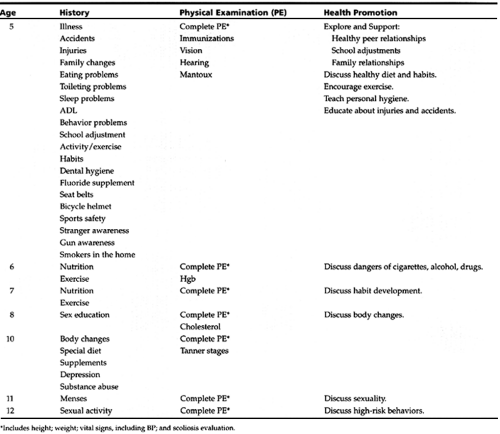
The American Academy of Pediatrics (AAP) recommends that school-age children receive a complete history and physical examination at ages 5, 6, 8, 10, 11, and 12 years. Additional visits may be necessary for children who have some variations from normal (AAP, 1997). When the history and physical examination are complete, it is important to ask the child if he or she has any questions. Table 11-1 provides critical foci for history, physical examination, and health promotion.
 |
History Topics
School-age children are valuable participants in providing the history. Providers should direct questions to both parent and child and ask both what their concerns are at each visit. In the late school-age years, it may be appropriate to take a history from the child privately as well as a history from the parent.
Physical Health
The following are questions to ask:
What is the child’s immunization status?
Have there been any illnesses, accidents, injuries, or visits to emergency departments?
Have you noticed any body changes? Has menses begun?
Do you have any concerns about your body?
Are you taking any medications?
Can you see the blackboard, or do you have any trouble reading?
Are there any problems with hearing?
Do you brush your teeth and floss at least daily and have regular dental checkups? Do you have any cavities or dental problems? Do you have fluoride in your water? Is your water source municipal or well?
Mental Health
The following are questions to ask:
Are you mostly happy or mostly sad?
What things make you happy and sad?
Are you worrying about anything?
Are you angry with anyone or about anything?
On a scale of 1 to 10, how do you get along with your parents and siblings?
Are there any problems with peers?
Do you ever think of hurting yourself or others?
Have there been discussions between parent and child regarding sexuality?
Diet
The following are questions to ask:
What do you eat during the course of the day? Give me an example of a typical meal.
What are some of your snack foods?
Do you eat between meals?
Do you eat in front of the television?
What do you drink?
How much caffeine, sugar, or artificially colored or sweetened drinks do you consume?
How much milk do you drink each day? What type of milk is it: whole, low fat, or skim?
What are the healthy foods you eat?
What are the “junk foods” you eat?
What foods do you refuse to eat?
Do you take any vitamins or other dietary supplements?
How do you feel about your weight?
Have you tried alcohol? Have you tried cigarettes?
Do you eat in fast food restaurants?
Are you a vegetarian or on any other special diet?
Habits and Physical Activity
The following are questions to ask:
Do you have any habits (eg, nail biting, thumb sucking, tics, mannerisms, compulsions)?
What physical activity do you get during the day?
Do you play sports? If so, which ones, how many times a week, and what time of the year?
Sleep
The following are questions to ask:
Are there any sleep problems (eg, difficulty getting to sleep, waking during the night, sleepwalking, nightmares, night terrors, late riser)?
What time do you go to bed?
What time do you get up?
Are there battles about bedtime?
Do you snore or have difficulty breathing during the night?
Elimination
The following are questions to ask:
Is the child completely toilet trained? Are there any problems with accidents, enuresis, or encopresis?
Do you have any problems with constipation or diarrhea? If so, are you using any medications or enemas?
Social
The following are questions to ask:
Who lives in the house?
If parents are divorced or separated, what are the arrangements for visitation?
Do both parents work? Are there any other caretakers?
Do you have a best friend?
What do you like best about school?
Are there any specific difficulties?
How many days have you missed from school this year?
How did things go at the last parent–teacher conference?
What do you do after school and on weekends?
What do you read? What are your hobbies? Do you belong to any groups?
Are there any behavior problems (eg, fighting, lying, stealing, sibling conflict, mood swings, aggression, defiance)?
• Clinical Pearl
The following are important questions to ask:
How many hours are spent watching television or playing video games per day? What do you watch or play?
How many hours are spent on the computer? What kind of computer use is usual?
To what kind of music do you listen?
Are there pets in the house?
Are there smokers in the house?
Are there guns in the house? If so, are guns and ammunition stored separately and in locked locations?
Safety
The following are questions to ask:
Do you wear a seat belt at all times?
Do you wear appropriate safety equipment for all sports (helmets and pads)?
Do you know how to swim? Are you supervised when you swim?
Do you know how to dial 911?
Have there been family discussions about alcohol, smoking, and drug use?
Do you know what to do if approached by a stranger?
Do you know the difference between “good touch and bad touch?”
Physical Examination
School-age children should be “old hands” at visits to their providers. They understand the concrete operation of a physical examination and want to cooperate. The provider should praise children for their successful participation and reward them for cooperation. Each visit should be an opportunity to build the child’s self-esteem.
Approach to Examination
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


