disability for work, household chores, and social activities reported by most migraineurs (3.3)5. According to the World Health Organization, migraine ranks among the top 20 causes of disability, ranking 12th for women and 19th for both genders combined6.
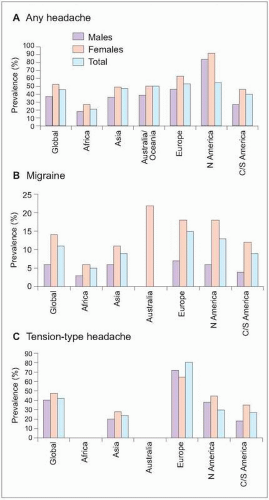 3.1 Prevalence of current headache in adults. Worldwide headache prevalence was estimated using a literature review of population-based headache studies. Since some studies provided data on male and female genders, while others reported for males and females combined, headache prevalence for all patients in some cases is reported to be less than for either males and females, e.g. total headache in North America (A). In other cases, prevalence for the total population is nearly the same as for females alone, e.g. total headache in Australia/Oceania (A). Despite these flaws, general regional headache trends are provided with these data. Current headache affects about half of the population in Asia, Australia, Europe, and North America, with only about 20% affected in Africa. Migraine in the total population is most prevalent in Europe (15%) and least prevalent in Africa (5%) (B). Among regions reporting tension-type headache, tension-type headache is similarly most common in Europe (80%) and least common in Asia and the Americas (20-30%) (C). (Based on Stovner LJ, et al., 20071.) |
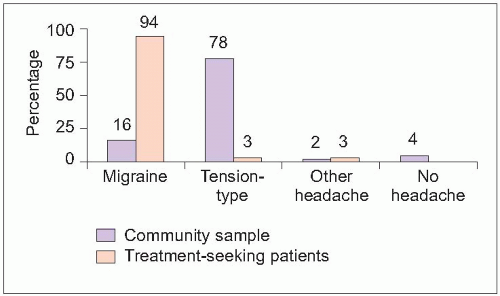 3.2 Comparison between prevalence of migraine and tension-type headache in the general population and in patients seeking treatment for headache. Community figures represent lifetime prevalence of headache. Treatment-seekers were 1,203 patients seeking care for headache as a primary or secondary complaint in 15 countries. A total of 128 clinical practices were utilized, 93% of which were primary care facilities. An international headache expert panel reviewed diagnoses using diary assessment and determined that the vast majority of patients had migraine. Although migraine occurs in only 16% of the general population, 94% of treatment-seeking patients have migraine. (Based on Rasmussen BK, et al., 19913; Tepper SJ, et al., 20044.) |
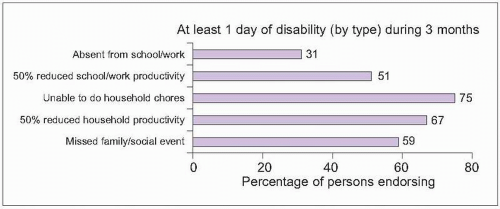 3.3 Migraine-related disability during the preceding 3 months was evaluated in a community survey of 29,727 migraineurs ≥12 years old in the American Migraine II study. Nearly one in four households surveyed had at least one member with migraine. Ninety-one percent of migraineurs reported functional impairment with their headaches. Severe headache caused substantial impairment in activities or bed rest in 53%. Most patients had experienced impairments in work, household, and social activities due to migraine in the previous 3 months. (Based on Lipton RB, et al., 20015.) |
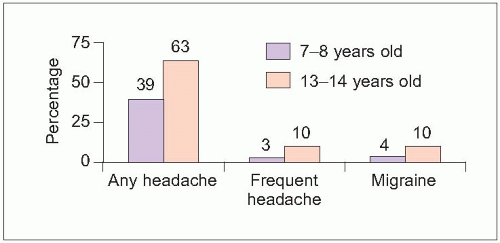 3.4 Pediatric headache. A survey of 5,586 households in Germany produced important data about pediatric headache occurring in the preceding 6 months. A total of 53% of children (55% of girls and 52% of boys) reported any headache in the previous 6 months, with headaches more common in adolescents than younger children (P<0.001). Frequent recurring headache (≥1 episode/week) and migraine were also more common in adolescents (P<0.001). (Based on Kröner-Herwig B, et al., 20077.) |
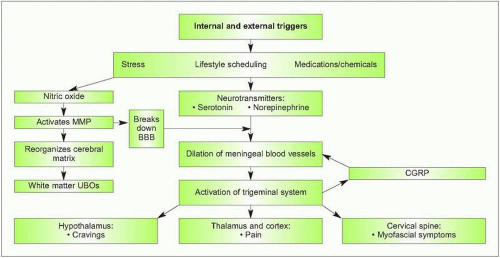 3.5 Neurovascular model of migraine. Michael Moskowitz developed the neurovascular model of migraine to explain important relationships between vascular and neural structures in the pathogenesis of migraine. Although specific mechanisms have not been uncovered, exposure to internal and external triggers (including stress, changes in sleep and eating habits, and hormonal cycling) results in alterations in signalling from a variety of important neurotransmitters (including nitric oxide, serotonin, and norepinephrine). All of these compounds activate vascular dilation. Dilated intracranial, extracerebral blood vessels result in a perceived throbbing sensation and increased blood flow. More importantly, neurons surrounding these blood vessels become stretched, resulting in activation of neural pathways and triggering of the trigeminal system. Once the trigeminal system is activated, signals travel in several directions. Antidromic signals travel back to the meningeal vessels causing a positive feedback loop to perpetuate vascular dilation and trigeminal activation; this is mediated by calcitonin gene-related peptide (CGRP), a target of new migraine medications. The trigeminal system also activates the hypothalamus, possibly resulting in migraine-related cravings. Activation of cervical trigeminal structures may facilitate transmission to somatic neurons, resulting in muscle contraction. Signals also travel to the thalamus and cortex to relay pain messages. Nitric oxide also activates matrix metalloproteases (MMPs), important compounds for brain development and plasticity. MMP-9 is linked to opening of the blood-brain barrier (BBB) and has an important role in the pathogenesis of brain ischemia and possibly migraine. Cortical spreading depression at the onset of migraine results in upregulation of MMP-9. This effect occurs early (within 15-30 minutes) and is prolonged (>48 hours)9, causing breakdown of the BBB, edema, and vascular extravasation. These changes in brain fluid status may explain the occurrence of nonspecific, unidentified bright objects (UBOs) in the white matter on magnetic resonance imaging studies in about 30% of migraineurs. These effects may also help explain how medications and neurotransmitters outside the BBB can gain access to the brain during a migraine. |
Table 3.1 Common causes of head pain | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
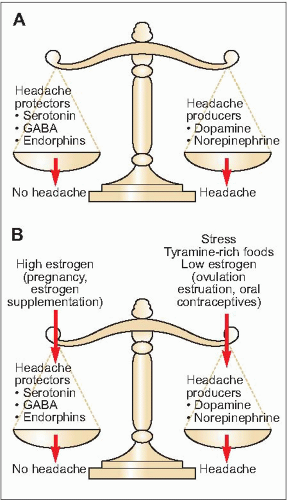 3.6. Neurochemical balance in chronic headache. Susceptibility to a headache episode depends on a balance between headache-protecting neurotransmitters (serotonin, GABA, and endorphins) and headache-provoking neurochemicals (dopamine and norepinephrine). When concentration and activity of headache protectors outweigh headache producers, the patient is less susceptible to headache episodes (A). Exposure to common headache triggers results in changes in levels and activity of a variety of neurotransmitters (B). Stress, the most common trigger, increases headache producers. Elevated estrogen increases headache protectors, reducing headache risk, while decreases in estrogen levels increase dopamine and norepinephrine, increasing headache susceptibility. In some patients, their scale is usually balanced toward increased headache susceptibility, so few additional triggers will activate a headache episode. Preventive therapies may help achieve and maintain a more favourable neurotransmitter balance. |
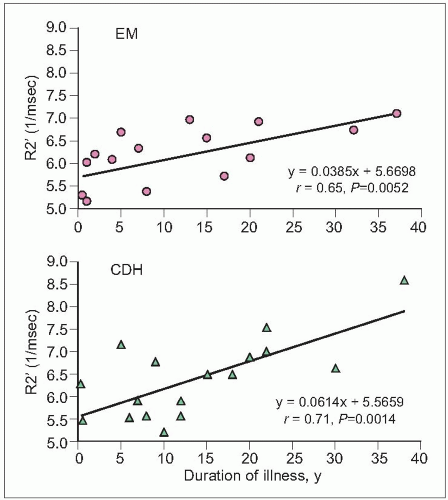 3.7 Iron deposition in migraine. Periaqueductal gray iron homeostatis was evaluated in patients with episodic migraine (EM, N=17), migraine transformed into chronic daily headache (CDH, N=17), and no headaches (N=17). Magnetic resonance imaging transverse relaxation values showed increased R2′ values in migraineurs, denoting increased iron deposition (EM=6.11, CDH=6.36, controls=4.33). There were no differences between migraine with and without aura. As seen in the graphs, migraine duration correlated with iron deposition for both EM and CDH. (Based on Welch KM, et al., 20018.) |
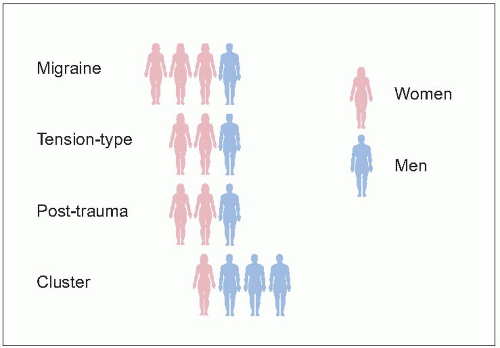 3.8 Gender distribution of chronic headaches. When tested with experimental pain, women have a lower pain threshold and pain tolerance than men, resulting in increased sensitivity to painful stimuli. Women tend to perceive painful signals earlier and more acutely than their male counterparts. This increased sensitivity to pain may explain the increased prevalence of many painful conditions, including headache, in women. Most common recurring headaches occur more frequently in women. Although men are more likely to experience head injury, post-traumatic headaches occur more often in women. Historically, cluster headache has been considered a ‘man’s headache’, with medical books often noting a 6:1 male predominance. While cluster headache is still more common in men, estimates over the last few decades show that the male predominance of cluster headache has decreased to 2-3:1. Researchers speculate that lifestyle changes, such as increased use of nicotine and alcohol, may have contributed to this increasing prevalence of cluster headache in women. |
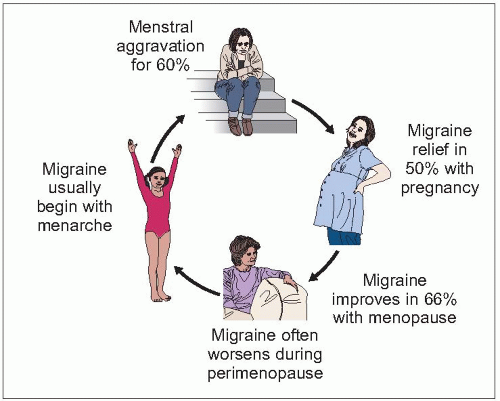 3.9 Lifetime patterns of migraine in women. In general, cycling estrogen acts as an important activating trigger to initiate migraine in women, with headaches aggravated whenever estrogen levels drop from a high to a low level, such as with menstruation or after delivery. Persistently elevated estrogen (such as with pregnancy) or lack of cycling (after menopause) tends to reduce migraine susceptibility. Women often notice an unexpected worsening of migraine in the perimenopausal period when they are also experiencing other somatic symptoms, like hot flashes. Migraine also tends to worsen after surgical menopause with hysterectomy/oophorectomy, while improving with spontaneous menopause, suggesting a possible role of ageing in migraine improvement. |
 3.10 A simple bedside fundoscopic examination with a hand-held ophthalmoscope is an essential part of the headache evaluation. This test can be performed within seconds and provides a window to the brain and blood vessels. Blurring of the vessels, as seen in this image, typically indicates increased intracranial pressure. Although MRI and CT scans identify many serious causes of headache, they do not identify all causes of increased intracranial pressure. For example, patients with increased intracranial pressure due to benign intracranial hypertension (pseudotumor cerebri) often have a normal imaging study even though their pressure is dangerously high. Failure to identify these patients can result in significant visual loss. (Photo courtesy of Rock Heyman, MD.) |
and radiographic studies in chronic headache patients should be targeted to specific disease states. MRI reveals nonspecific white matter abnormalities in about one in three migraineurs, with prevalence slightly higher in patients with migraine with aura (3.12)12.
Table 3.2 Features suggesting secondary headache | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 3.3 Laboratory testing for chronic headache | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
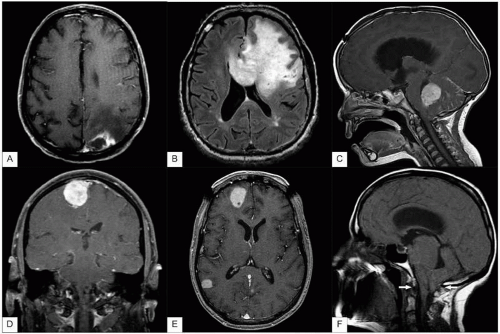 3.11 MRI scans of patients wiht secondary headache. While patients are often concerned that head pain signifies serious intracranial structural pathology, headache is typically a secondary complaint among patients with structural lesions. A: Occipital lobe abscess. Brain abscess may occur after infections of cranial structures (e.g. otitis media, mastoiditis, or sinus or dental infection), trauma, or via blood transfer from systemic infection. Risk increases in patients with right-to-left heart shunts or compromised immune systems. Patients typically present with headache, changes in mental status, seizure, and focal neurological symptoms or signs, such as visual deficits in this patient. B: Glioblastoma multiforme is the most common and aggressive primary brain tumor. Initial symptoms often involve memory, personality, and cognition, as well as headache, seizure, and focal deficits. C: Medulloblastoma is a glioma originating in the cerebellum or posterior fossa, most commonly affecting young children. Males are affected about twice as often as females. Symptoms include listlessness, headache, vomiting, gait imbalance, dizziness, and double vision. D: Meningioma is the most common benign tumor in adults, affecting women twice as often as men. Meningiomas arise from arachnoidal cells, forming an extra-axial brain mass, with the base attached to the dura. Symptoms include seizures and focal neurological deficits, in addition to headache. E: Cerebral metastases are the most common brain tumors, most commonly from primary sites in the lung, breast, and colon. Metastases are typically located at the gray-white matter junction. The most common symptoms are headache, focal weakness, and mental status changes. Seizures and other focal neurological deficits may also occur. The apparent symmetrical frontal skull defects are artifacts from a cranial frame used for a stereotactic procedure. F: Arnold-Chiari malformation is a downward displacement of the cerebellar tonsils and medulla through the foramen magnum. The arrows demonstrate the opening for the foramen magnum. Symptoms typically occur when the cerebellar tonsils are displaced at least 3 mm below the foramen magnum. Symptoms may include headache, neck pain, dizziness/vertigo, difficulty swallowing, and motor weakness. (A-E courtesy of Clayton A. Wiley, MD, PhD; F courtesy of Rock Heyman, MD.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





