33 Head and Facial Trigeminal Neuralgia
Trigeminal neuralgia is a disease characterized by brief, stereotypical episodes of lancinating pain in the trigeminal nerve distribution on a single side. The vast majority of cases affect either the second or third division (V2 or V3), alone or in combination. In only 4% to 5% of patients, symptoms occur solely in the first division (V1, Table 33-1). Historically, trigeminal neuralgia is considered one of the most painful disorders known to mankind. The name “tic douloureux” was coined by Nicholaus Andre, referring to the spasm of the face that follows an attack of pain. John Fothergill first codified the clinical characteristics of the disease in his paper “On a Painful Affliction of the Face,” which was published in London in 1775.
Table 33-1 Distribution of Pain in Trigeminal Neuralgia
| Distribution | % |
|---|---|
| V1 alone | 4 |
| V2 alone | 17 |
| V3 alone | 15 |
| V2 + V3 | 32 |
| V1 + V2 | 14 |
| V1 + V2 + V3 | 17 |
Afflicted patients typically describe the pain as electric, shooting, and shocklike. The pain occurs in attacks, each of which lasts only seconds or less; however, attacks tend to cluster so that pain-free episodes may not be appreciated.1,3 Pain can be precipitated by light mechanical stimulation to small trigger zones in the face or oral mucosa. Frequent triggers include light touch, wind, brushing teeth, speaking, eating, and drinking. There may be ipsilateral muscle spasm described in the condition termed tic douloureux. The disease typically takes a sporadic course, with remissions that may last months or even years. Most people have normal neurological examinations and are symptom free between attacks. The annual incidence is between 4 and 5 in 100,000. It typically affects people older than 50 years, although instances of the disease in young adults and even children have been reported. There is a slight female predominance.2 Strong environmental or genetic predisposing factors are not apparent.
Anatomy
The nerve then separates into three divisions (Fig. 33-1), each of which can be compressed by local inflammatory conditions or primary neoplastic or metastatic lesions. The ophthalmic nerve (V1) courses anteriorly through the cavernous sinus, where it is accompanied by cranial nerves III, IV, VI, and V.2 It exits the skull through the superior orbital fissure and passes into the orbit. From there, it divides to supply the eyeball, lacrimal glands, conjunctiva, part of the nasal mucosa, and skin of the nose, eyelid, and forehead.
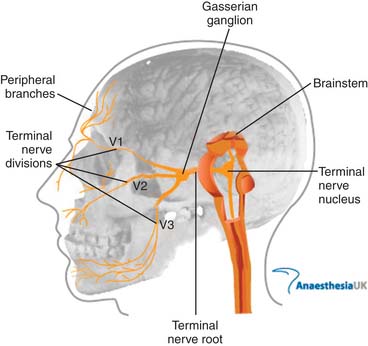
Figure 33-1 Anatomy of the trigeminal nerve.
Image from http://www.frca.co.uk/images/trigeminal_nerve.jpg, accessed 2010, March 14, courtesy of AnaesthesiaUK.
The mandibular nerve (V3) exits the skull more proximally through the foramen ovale and passes into the masticator space. It supplies the lower third of the face as well as the tongue and floor of the mouth and jaw. The motor root, which bypasses the gasserian ganglion but then rejoins the mandibular nerve provides innervation to the muscles of mastication (see Fig. 33-1).
Pathophysiology
Although Jannetta and colleagues showed that surgical decompression of the nerve root can effectively alleviate the symptoms of trigeminal neuralgia, a pathophysiologic connection between trigeminal nerve compression and the intermittent nature of the disease has not been well elucidated.4 A disease mechanism must also explain how nonnoxious peripheral mechanical stimuli trigger pain within different regions of the face. In a number of patients who undergo surgical exploration, no compressing vessel or lesion has been identified.
Pathologic rhizotomy specimens have demonstrated focal loss of myelin with close apposition of the demyelinated axons.5,6 Hilton found five patients without microvascular compression who did not show demyelinating features. In the study by Devor and colleagues, 1 of the 12 patients was not found to have vascular compression, and the rhizotomy specimen from this patient showed only “modest dysmyelination”.
Devor and his colleagues proposed their “ignition hypothesis” by which nerve compression leads to an increase in neuronal activity and reduced firing thresholds.6 In support of this hypothesis, Vos and colleagues showed in rats that mild compression of the infraorbital nerve produces a facial pain syndrome.7
Diagnosis
The White and Sweet criteria for trigeminal neuralgia8 were a major advance that facilitated research and enabled early and accurate clinical recognition of the syndrome (Tables 33-2 through 33-4). The criteria were incorporated, largely unchanged, into the official research diagnostic framework criteria published by the International Association for the Study of Pain (IASP)9 and the International Headache Society (IHS).3
Table 33-2 Sweet Diagnostic Criteria for Trigeminal Neuralgia
From White JC, Sweet WH: Pain and the Neurosurgeon. Springfield, Ill. Charles C Thomas, 1969.
Table 33-3 ICHD Criteria for Classic Trigeminal Neuralgia
ICHD, International Classification of Headache Disorders.
Table 33-4 ICHD Criteria for Symptomatic Trigeminal Neuralgia
ICHD, International Classification of Headache Disorders.
The current IHS criteria (International Classification of Headache Disorders II [ICHD-II])3 establishes trigeminal neuralgia as a discrete clinical diagnosis under the general classification of “cranial neuralgias and central causes of facial pain” (ICHD-II diagnostic code 13). The diagnosis ‘‘trigeminal neuralgia’’ (diagnostic code 13.1) replaces the earlier term, tic douloureux. ICHD-II further subdivides trigeminal neuralgia into ‘‘classic trigeminal neuralgia’’ and ‘‘symptomatic trigeminal neuralgia.’’ Classic trigeminal neuralgia (Table 33-3) is the most common idiopathic form of the disorder (although it also includes cases associated with vascular compression). Classic trigeminal neuralgia is defined as ‘‘a unilateral disorder characterized by brief electric shocklike pains, abrupt in onset and termination, limited to the distribution of one or more divisions of the trigeminal nerve. Pain is commonly evoked by trivial stimuli including washing, shaving, smoking, talking and/or brushing the teeth (trigger factors) and frequently occurs spontaneously. Small areas in the nasolabial fold and/or chin may be particularly susceptible to the precipitation of pain (trigger areas). The pains usually remit for variable periods.’’ The ICHD-II specific diagnostic criteria for classic trigeminal neuralgia are listed in Table 33-3. Symptomatic trigeminal neuralgia has the same key features of trigeminal neuralgia but results from another disease process (such as multiple sclerosis or a cerebellopontine angle tumor). Symptomatic trigeminal neuralgia is defined by IHS as ‘‘Pain indistinguishable from classic trigeminal neuralgia but caused by a demonstrable structural lesion other than vascular compression.’’ The ICHD-II diagnostic criteria for symptomatic trigeminal neuralgia are listed in Table 33-4.
Because a significant percentage of patients have symptomatic trigeminal neuralgia resulting from another disease process, diagnostic brain imaging studies should be part of the initial evaluation of any patient with trigeminal neuralgia symptoms.10,11 The study should visualize the anatomic landmarks around the trigeminal (gasserian) ganglion and the cerebellopontine angle. Although a routine brain CT scan is usually adequate to screen for a cerebellopontine tumor, an MRI scan often better demonstrates multiple sclerosis plaques and the anatomic relationships of the trigeminal root. High-resolution imaging techniques are also increasingly able to visualize subtle vascular anomalies that may be the source of root compression in certain patients with classic trigeminal neuralgia. Other diagnostic studies, such as blood studies, lumbar puncture, and evoked potentials, are generally not necessary.
Medical Treatment
Carbamazepine has been the mainstay of medical treatment for trigeminal neuralgia for many years.12 A Cochrane review on this subject confirmed that carbamazepine with a number needed to treat (the number of people who would need to be treated to see benefit in one person) of 2.5 was the recommended initial treatment for trigeminal neuralgia.13 Antiepileptic drugs were first used in the treatment of trigeminal neuralgia when Bergouignan in 1942 noted that the anticonvulsant phenytoin effectively controlled attacks of pain in the condition.14 Studies on various antiepileptic drugs have revealed that although carbamazepine and lamotrigine are superior to placebo in trials, most others drugs thought to be useful do not have trials to support their use.15 Baclofen is another choice for monotherapy for trigeminal neuralgia as was evidenced in data from Fromm and colleagues.16 In many instances where carbamazepine is not tolerated, initial therapy with baclofen has been successful.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



{kind=link}