HEAD (ALSO EYE, EAR, NOSE, THROAT, AND MOUTH)
HEADACHE
Tension or fatigue headache is characterized by throbbing pain in the temples, over the eyes, and in the posterior neck and shoulder muscles. It can be treated with rest, sunglasses, and moderate pain medication, such as aspirin or acetaminophen every 3 to 4 hours. Sometimes, applying warm packs or massage to tense muscles relaxes them and helps relieve the pain.
Migraine headache is generally more severe. It is defined as episodic attacks of headache lasting 4 to 72 hours and characterized by at least two of the following: moderate to severe intensity, one-sided pain, throbbing or “pulsating,” and worsening with movement. In addition, there is nausea or vomiting (which may be treated with metoclopramide [Reglan] 10 mg by mouth or with ondansetron [Zofran] 4 mg oral dissolving tablet), and aversion to light or sound. Migraine headache is currently thought to be caused by painful dilation of small arteries in the head. Migraine headaches have many variations, which may include stuffy or runny nose and weakness of an arm or a leg. Some people experience an “aura” before the “classic” migraine headache, in which they may smell strange odors or see flashing lights. Others develop tunnel vision—diminished peripheral vision. The headaches are characterized as excruciating, pounding, or explosive. Occasionally they will respond to nonsteroidal antiinflammatory medications, such as ibuprofen, but often require stronger pain medications and sometimes may need to be treated with narcotics. A person suffering from a migraine should be placed in a quiet, dark area to minimize external stimuli. He should be encouraged to drink enough liquid to treat or prevent dehydration and offered ibuprofen, acetaminophen, or aspirin. Caffeine may be helpful.
Specific antimigraine medications include the “triptans,” such as sumatriptan (Imitrex), naratriptan (Amerge), rizatriptan (Maxalt), and zolmitriptan (Zomig). These medications should be given as early as possible in the course of the headache to achieve maximal effectiveness. Other medicines that are effective include propranolol or metoprolol, amitriptyline, methysergide, flunarizine, and prochlorperazine (Compazine) given with diphenhydramine (Benadryl). Ergotamine drugs (such as dihydroergotamine mesylate [Migranal] nasal spray) directly constrict arteries; these should only be used under the direct supervision of a physician, since they may worsen the effects of certain types of migraines. If an oxygen (see page 431) tank is available, the victim may get some relief by breathing 10 liters per minute by face mask. An elderly person with a severe migraine, which may be confused with a stroke (see page 144), should seek immediate medical attention. A migraine headache may be precipitated by lack of sleep, high altitude, emotional stress, cyclical hormone changes, noxious odors, and certain ingested substances (such as caffeine and monosodium glutamate). Therefore, the migraine sufferer should seek to obtain regular sleep (go to bed and wake up at the same times every day), rest, and meals (do not skip or delay); limit caffeine consumption to the equivalent of two cups of coffee or two 12-ounce sodas per day; avoid tobacco products; avoid known personal triggers (e.g., red wine); practice relaxation techniques; and strive to maintain fitness through regular exercise and dietary discretion. For certain sufferers, a neurologist may prescribe topiramate (Topamax) to be taken between episodes of migraine to reduce the frequency of headaches.
Sinus headache is associated with sinus infection (see page 194) and is typified by fever, nasal congestion, production of a foul nasal discharge, and pain produced by tapping over the affected sinus(es). It should be treated with an oral decongestant (pseudoephedrine), nasal spray (Neo-Synephrine 0.25% or Afrin 0.05%), an antibiotic (azithromycin, amoxicillin-clavulanate, erythromycin, or ampicillin) if an infection is present, and warm packs applied over the affected sinus(es).
Subarachnoid hemorrhage is bleeding that occurs, usually suddenly, from a leaking blood vessel (commonly an aneurysm) underneath the thin tissue layer that surrounds the brain and spinal cord. The headache is usually sudden in onset, described as “the worst headache of my life,” and may be associated with a fainting spell, altered mental status, seizure, and collapse. If a person suffers a subarachnoid hemorrhage and remains awake, he may complain of a stiff or painful neck with or without back pain about 2 to 4 hours after the bleed. Anyone who complains of a severe headache after extreme physical straining (such as weight lifting or a difficult bowel movement) or who collapses suddenly after reporting a headache should be suspected to have suffered a subarachnoid hemorrhage and be brought rapidly to a hospital.
Meningitis, an infection that involves the lining of the brain and spinal cord, is a true emergency. The headache of meningitis is severe, and often accompanied by nausea, vomiting, photophobia, fever, altered mental status, and weakness. A purplish skin rash indicates infection with the bacteria Neisseria meningitidis, a particularly fulminant and contagious form (“meningococcal”) of infectious meningitis. The classic signs of meningitis are a stiff neck with a fever. The victim demonstrates extreme discomfort when the chin is flexed downward against the chest, and may complain that the pain also occurs in the back (along the course of the spinal cord). It is important to note that an infant can suffer meningitis without a stiff neck and may present only with poor feeding, fever, vomiting, seizures, and extreme lethargy (“floppy baby”). If meningitis is suspected, the victim must be evacuated rapidly. If antibiotics are available, the recommendations currently given to doctors for antibiotics are as follows: age 16 to 50 years, vancomycin plus either cefotaxime or ceftriaxone; age greater than 50 years, vancomycin plus either cefotaxime or ceftriaxone, as well as ampicillin.
Giant cell arteritis is a type of inflammation that occurs in elders that can affect the temporal artery, which travels in a path along the sides of the scalp over the ears (temples). The associated headache may be quite severe and accompanied by thickened and tender arteries that may be noticeably enlarged with or without overlying reddened skin. Pulses may or may not be appreciated in these arteries, and the victim may have pain radiating down the side of the face as low as into the jaw. Permanent partial or complete loss of vision may occur in one or both eyes, which makes this condition an emergency. This condition is frequently associated with the disorder polymyalgia rheumatica. The immediate treatment is administration of a corticosteroid, such as prednisone 40 to 60 mg by mouth each day until a physician can evaluate the patient.
A headache that is atypically severe or prolonged may represent a serious problem, such as accelerated (out of control) high blood pressure (hypertension), brain tumor, infection, glaucoma, blood clot within the brain, carbon monoxide poisoning, inflammation of the temporal artery, or hemorrhage. The victim should be evaluated by a physician at the earliest opportunity. If a person develops a severe headache associated with a fainting spell or stiff neck, or is known to suffer from high blood pressure, keep him as calm as possible and urgently seek assistance. If high blood pressure is known to be the problem, and the victim is taking antihypertensive drugs, he should be advised to avoid using medications or other substances that might counteract the effects of his antihypertensives. These include ephedra, phenylephrine, certain herbal supplements (such as ginseng and yohimbine), appetite suppressants, anabolic steroids, and certain nonsteroidal antiinflammatory drugs.
In general, particularly worrisome headaches include a single headache that is the “first” or “worst” of a person’s life; headache with a fever that is not explained by an obvious illness; headache with vomiting that is not explained by an obvious illness; headache associated with a neurologic sign, such as weakness or altered speech; headache associated with altered mental status; headache associated with neck pain when the chin is flexed to the chest; progressively worsening headache; sudden headache in an elder; headache in someone suffering from cancer; headache after a blow to the head; headache following an episode of loss of consciousness; or headache in someone suffering from immunosuppression.
EAR
Earache
An earache may be caused by infection, injury, or a foreign body in the ear. For a discussion of ear squeeze (barotitis) that occurs with scuba diving, see page 404.
Ear Infection
Ear infection can be either internal (otitis media) or external (otitis externa) to the eardrum (tympanic membrane) (Figure 107).
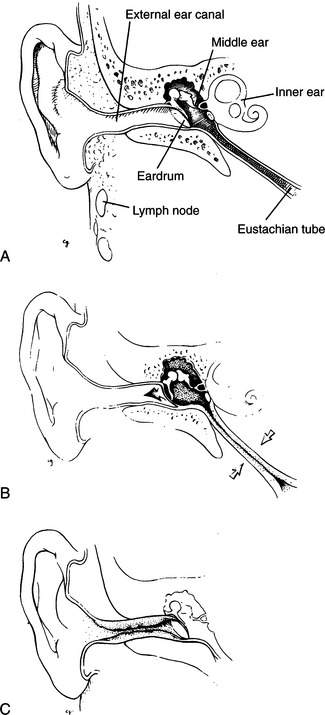
Otitis media. Infection may occur that reddens and inflames the eardrum and causes blood, serum, or pus to collect behind the drum (see Figure 107, B). With otitis media (middle ear infection), there is no drainage from the external ear canal (unless the eardrum ruptures, which is unusual in an adult, although more common in a child) and the victim has a fever, often with a sore throat. In many cases, the victim has a history of prior infections. Most often, otitis media occurs in children; when it occurs in an adult, it may be associated with a sinus infection or functional obstruction of the eustachian tube (the pressure-release mechanism from the middle ear into the throat). A young child can rapidly become severely ill from otitis media; an infant may develop meningitis (see page 174) following an ear infection. It is interesting to note that children who chew sugarless gum containing xylitol (or who ingest syrup or granules containing xylitol), which is derived from birch trees, may have fewer ear infections. This is supposedly because xylitol inhibits the growth of certain bacteria that cause the infections. It is reasonable to advise children prone to ear infections to avoid sugar-containing gum or candies.
Although many cases of otitis media in children are caused by viruses, such as respiratory syncytial virus, and resolve without antibiotic treatment, if you are distant from physician care and suspect otitis media, treat the child victim with an antibiotic. Adults and children should be treated with amoxicillin (80 to 100 mg/kg [2.2 lb] of body weight per day in three divided doses), amoxicillin-clavulanate (same dose of the amoxicillin component as for amoxicillin), cefdinir (14 mg/kg once daily or in 2 divided doses), cefpodoxime (10 mg/kg once daily or in two divided doses), cefuroxime (15 mg/kg in two divided doses), or clarithromycin for 10 days, or with azithromycin for 5 days. An additional antibiotic choice for children is erythromycin-sulfisoxazole for 10 days. Other antibiotics that have been approved for treatment are cephalexin, cefprozil, loracarbef, and ceftibuten. Aspirin, ibuprofen, or acetaminophen should be used to control fever. To avoid Reye syndrome (postviral encephalopathy and liver failure), do not use aspirin to control fever in a child under age 17.
Otitis externa (swimmer’s ear). Ear infection, commonly from the bacterium Pseudomonas aeruginosa, that develops in the external ear canal (often noted in swimmers and divers who do not keep the canal completely dry) rarely involves the eardrum (see Figure 107, C). When the external canal is kept moist, it is easier for bacteria to invade the skin and cause infection. The earliest symptom may be itching. Subsequent symptoms include a white to yellow-green liquid or cheesy discharge from the ear, pain, and decreased hearing. Occasionally, the victim complains of exquisite tenderness when the earlobe is tugged or the jaw is moved and has tender, swollen lymph glands in the neck on the affected side. In a severe case, the victim may have a fever and appear toxic.
If the victim has only a discharge without fever or swollen lymph glands, he may be treated with ear drops, such as 2% nonaqueous acetic acid (VoSoL or Domeboro Otic). Household vinegar diluted 1:1 with fresh water or with rubbing (isopropyl) alcohol (approximately 70%) can be used as a substitute. These ear drops should be administered four to five times a day and may be retained with a cotton or gauze wick gently placed into the external ear canal, or by using an expanding foam ear sponge (such as a Speedi-Wick, Shippert Medical Technologies). To avoid injuring the eardrum, do not attempt to clean out the ear with a cotton swab or similar object. The solution should be retained in the ear for a minimum of 5 minutes with each application. If there is any suggestion that the eardrum may be punctured (e.g., the presence of bleeding), do not use this solution.
If the victim has a discharge with fever and/or swollen lymph glands, the ear drops should contain hydrocortisone (VoSoL HC); he should also be given oral ciprofloxacin, erythromycin, or penicillin. An ear drop that may be useful is ciprofloxacin with hydrocortisone (Cipro HC otic suspension). Another is ofloxacin otic solution (Floxin otic) 0.3%. These ear drops are used twice a day. If the discharge from the ear is gray or black, a fungal infection may also exist, in which case tolnaftate 1% solution may be added to the treatment regimen. Aspirin, ibuprofen, or acetaminophen should be used to control fever. To avoid Reye syndrome (postviral encephalopathy and liver failure), do not use aspirin to control fever in a child under age 17.
To prevent swimmer’s ear, the external ear canal should be irrigated with VoSoL, Domeboro Otic solution (2% acetic acid, aluminum acetate, sodium acetate, and boric acid) or diluted vinegar/alcohol (described above) after each scuba dive or immersion episode in the water. Keep the solution in the canal for a full 5 minutes before allowing it to drain.
Injury to the Eardrum
If something is poked into the ear, a hard blow is struck to the external ear, a diver descends rapidly without equalizing the pressure in his middle ear (see page 404), or a person is subjected to a loud explosive noise, the eardrum may be ruptured. This causes immediate intense pain and possibly loss of hearing, along with occasional nausea, vomiting, and dizziness. If the eardrum is ruptured, cover the external ear to prevent the ingress of dirt, and seek the aid of a physician. If debris has entered the ear, start the victim on penicillin or erythromycin by mouth. Do not put liquid medicine into the ear if you suspect that the eardrum is ruptured. If the dizziness is disabling, administer medicine for motion sickness (see page 440). Use appropriate pain medication.
EYE
Foreign Body under the Eyelid and Scratched Cornea; Corneal Ulcer
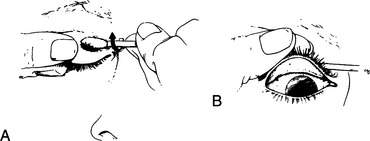
If a foreign body lodges on the cornea (the clear surface of the eye) without actual penetration of the eyeball, irrigate the eye copiously with an eyewash solution (use water if you do not have eyewash). If this is not successful, have the victim look downward, grasp his upper lid firmly by the eyelashes, and fold it up and inside out over a cotton swab (Figure 108). You can lightly grease the swab with antiseptic ointment to keep it from sticking to the skin. If you can see the foreign body on the undersurface of the upper eyelid, gently wipe it away with a cotton swab or piece of moistened cloth. If you do not see the object, check between the lower eyelid and the eyeball. After the inspection, pull down on the eyelashes to unfold the lid.
Once you have removed the object, if the victim still feels as if something is in his eye, he may have suffered a scratch on the cornea (corneal abrasion). In this case, it may help control the discomfort to patch the eye closed for 24 hours. However, never patch an eye closed if there is any sign of an active infection (pus or discharge). When the patch is removed, if there is residual pain, a gritty sensation, gooey discharge, or blurred vision, see a doctor as soon as possible. Tiny objects, such as the spine of a horse nettle (sand brier), can become embedded in the cornea and not be visible without the magnification available to an ophthalmologist.
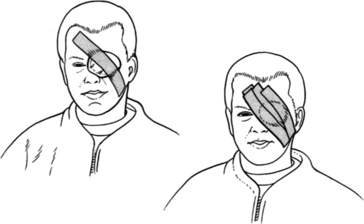
To patch an eye, a ½ in (1.3 cm) thick pad of soft cloth or bandage should be shaped to fit neatly over the eye socket, and affixed snugly to the face with tape or bandages extending across the patch onto the cheek below and the forehead opposite the affected eye (Figure 109). Prepackaged sterile elliptical eye pads are available. If only tape is available, the eyelids may be taped closed with a single small piece of tape.
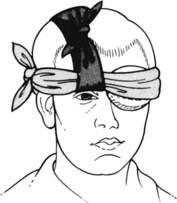
Another way to hold an eye shield, patch, or padding around the eye is with a cravat (see page 277). First, place a strip of cloth approximately 2 in (5 cm) wide and 15 in (38 cm) long over the top of the head front-to-back, so that the face-side end hangs over the uninjured eye, near the nose. Place the patch, pad, or shield over the eye and hold it in place with a cravat, which should be wrapped horizontally around the head and then tied in position on top of the hanging cloth strip. Make the first tie (single loop or half square knot) in the cravat behind the head and at the base of the skull, and keep wrapping it around, to complete the final tie (square knot) where the ends meet. If the final tie will be over an eye, shift the cravat. Pull up the ends of the hanging cloth strip and tie them at the top of the head; this should lift the cravat up off the uninjured eye (Figure 110).
Injured Eyeball
If the eyeball is perforated, there will be a combination of loss of vision (ranging from hazy vision to blindness), pain, excessive tearing, a dilated pupil, and visible blood in the eye. There may be gelatinous material extruding from the eye, and the pupil will be irregular or jagged in appearance. Do not attempt to rinse out the wound vigorously; remove obvious dirt and debris without placing any pressure on the eye. Close the eyelid gently and cover the eye with a protective shield. This can be fashioned by cutting gauze pads or soft cloth to the proper size, or by fashioning a doughnut-shaped shield with a cloth, cravat bandage, or shirt (Figure 111). Another good way to keep pressure off the eye is to cut an eye-sized hole in a stack of gauze pads and place the stack over the eye, taping or wrapping it in place. An eye shield can also be improvised by cutting off the bottom 2 in (5 cm) of a paper cup and taping it over the eye. Metal or plastic preshaped eye shields can be carried.



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


