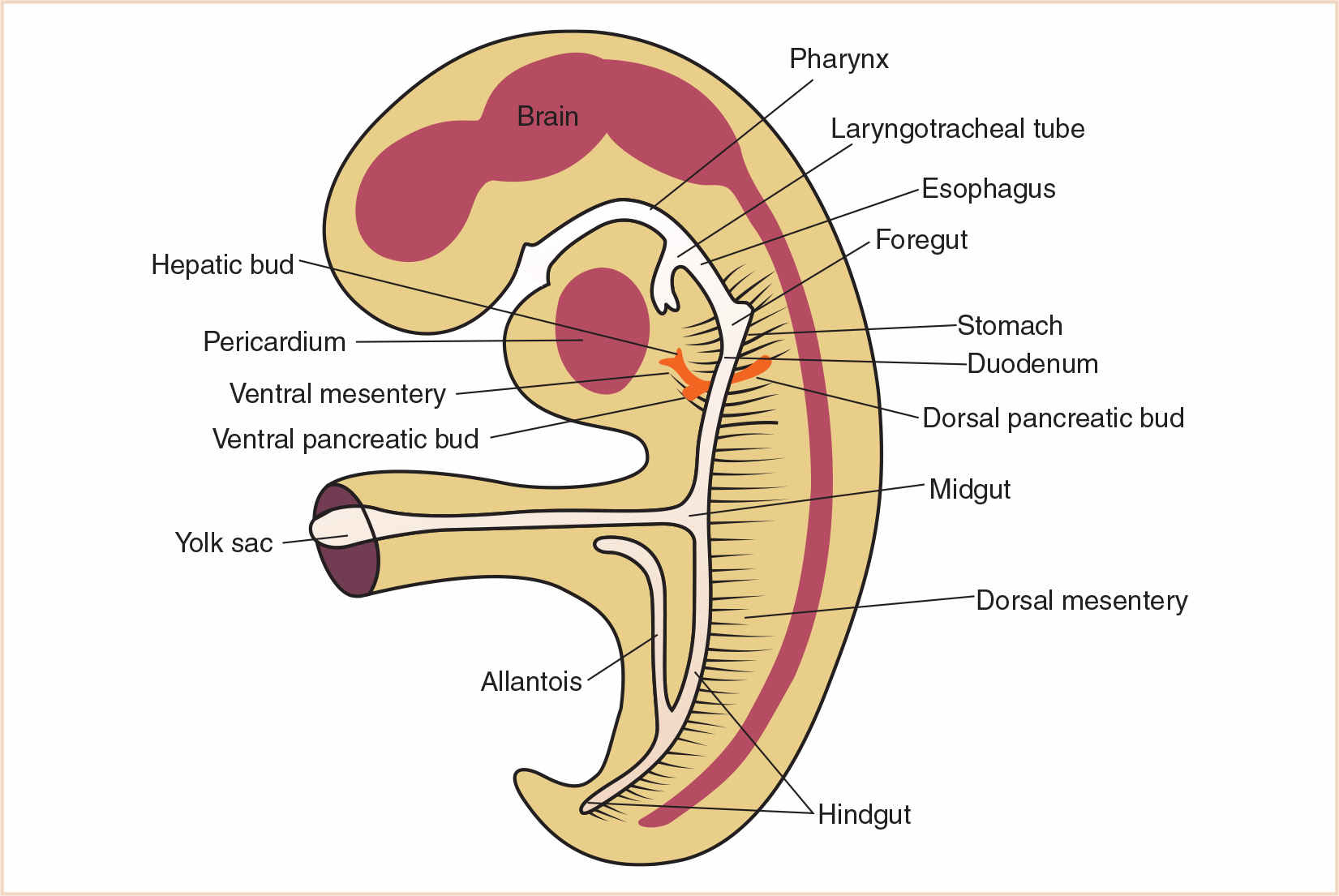
1. The endoderm is divided into the foregut, midgut, and hindgut based on its vascular supply.
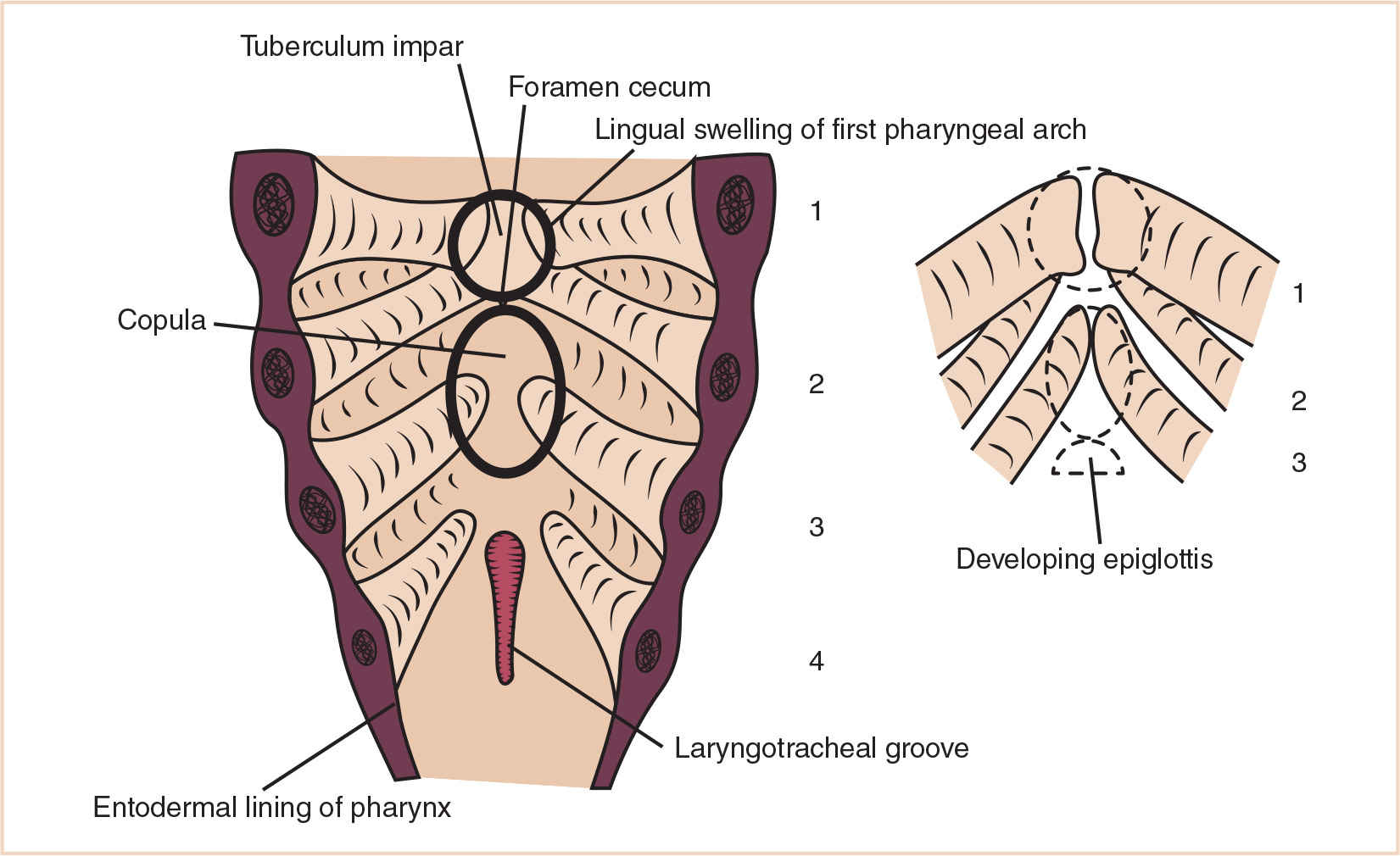
2. The tongue’s complex muscular and nervous innervation is a result of its development from branchial arches 1 to 4 as well as occipital myotomes.
3. While the cranial two thirds of the esophagus develop striated muscle from branchial arch mesenchyme, the caudal one third of the esophagus consists of smooth muscle derived from splanchnic mesenchyme.
4. The original main hepatic bud and its right and left branches ultimately form the common, right and left hepatic ducts as well as the right and left lobes of the liver. Abnormalities of development with any of these embryological anlage may result in stenosis, agenesis, or cystic malformations of the major ductal or vascular structures of the liver.
5. The small bowel caudal to the second half of the duodenum as well as the large bowel up to the left colic flexure is derived from the midgut, which lengthens so rapidly that it forms a loop attached to the vitelline duct, which becomes known as the omphalomesenteric duct.
6. Abnormalities of midgut formation may result in a Meckel’s diverticulum (in about 2% of people), a residual of the proximal portion of the vitelline duct, various degrees of patency of the omphalomesenteric duct, malrotations, stenoses, and atresias of the small bowel.
7. The anal canal and rectum are the locations of the most frequent gastrointestinal tract malformations.
8. Necrotizing enterocolitis with bowel perforation usually occurs within the context of a stressed premature infant with respiratory disease, sepsis, coagulopathy, and thrombocytopenia.
The endoderm gives rise to almost the entire length of the digestive system from mouth to anus, with mesodermal layers surrounding it and extending to the body wall. It is divided into the foregut, midgut, and hindgut based on its vascular supply (the foregut artery [which becomes the celiac artery], the midgut artery [the eventual superior mesenteric artery], and the hindgut artery [the eventual inferior mesenteric artery]) (Fig. 20.1).
THE FOREGUT
Mouth: Starting at the cephalic end of the gut, the stomodeum forms from an ectodermal depression adjacent to the most cranial portion of the endodermally-lined foregut. While the fusion of these two structures is prevented in the early embryo by the buccopharyngeal membrane, at about the 3rd week of development this membrane regresses.
Tongue (Fig. 20.2): A median swelling developing in the floor of the pharynx becomes invested laterally with mesenchyme from the first branchial arch, forming the anterior two thirds of the tongue. It is innervated by the lingual nerve (branch of the fifth cranial nerve) and the chorda tympani (branch of the seventh cranial nerve—taste). A second median swelling develops posterior to the first and becomes invested with mesenchyme from the second, third, and fourth pharyngeal arches. It is the ninth cranial nerve that provides sensation and taste to this more embryologically-complicated posterior third of the tongue. The muscles of the tongue are derived from occipital myotomes, which are innervated by the 12th cranial nerve. A transverse groove developing across the posterior third of the tongue gives definition to the initial tissue of the epiglottis, which then deepens to form the vallecula. A small opening which subsequently forms a caudally-migrating channel in the pharyngeal floor at the junction of the anterior two thirds and posterior one third of the tongue becomes the foramen cecum, leading to the formation of the thyroid gland.
Esophagus: The tubular structure of the cranial-most portion of the primitive foregut becomes divided by the tracheoesophageal septum into the more ventral trachea and the dorsal esophagus. The esophagus elongates along with the “descent” of the heart and diaphragm as the fetus grows. While the cranial two-thirds of the esophagus develop striated muscle from branchial arch mesenchyme, the caudal one third of the esophagus consists of smooth muscle derived from splanchnic mesenchyme.
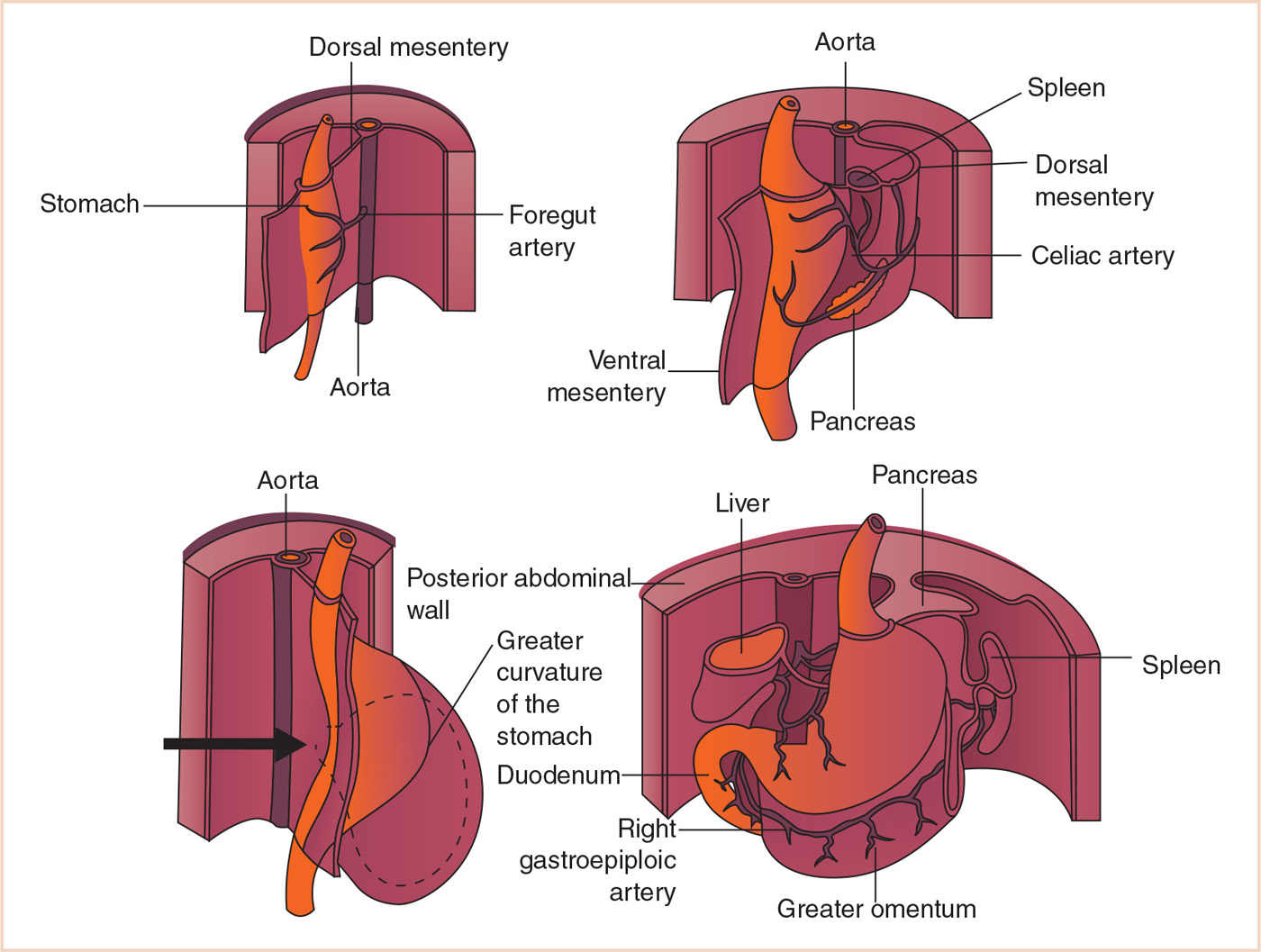
Stomach (Fig. 20.3): This dilated portion of the foregut becomes concave anteriorly and convex posteriorly as a result of differential growth along the ventral and dorsal mesentery. Ongoing growth of the stomach as well as adjacent growth of the liver results in stomach rotation, with the left surface rotating anteriorly and the right surface posteriorly. This also alters the position and eventual role of the ventral and dorsal mesenteries, which become the omental and peritoneal ligaments. In addition, this rotation forms the lesser sac posterior to the stomach.
Duodenum (Fig. 20.4): The duodenum is derived from the most caudal portion of the foregut and the most cephalic portion of the midgut. As the stomach rotates from left to right, the duodenum is forced to displace itself to the right as well; however, its second, third, and fourth portions remain fixed to the posterior abdominal wall via a residual of the dorsal mesentery, the ligament of Treitz.
Liver (Fig. 20.5): The liver and pancreas develop from an endodermal bud at the caudal end of the foregut that grows into the mesoderm of the septum transversum. While the endodermally-originated cells divide into left and right branches and grow into the mesenchyme, the mesoderm itself develops into vascular structures (paired umbilical and vitelline veins) which are broken up by endodermal cells into liver sinusoids. Meanwhile, the mesoderm of the septum transversum ultimately becomes the capsule of the liver and its connective tissue. The original main hepatic bud and its right and left branches ultimately form the common, right, and left hepatic ducts as well as the right and left lobes of the liver. Abnormalities of development with any of these embryological anlage may result in stenosis, agenesis, or cystic malformations of the major ductal or vascular structures of the liver.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


