Chapter 2 General Approach to Trauma Patients
3 How is the airway managed in trauma patients?
Airway management is discussed thoroughly in Chapter 14, but trauma patients can pose a unique set of airway management challenges. Maxillofacial, laryngotracheal, and neck injury; intracranial hypertension; hemodynamic instability; thermal injury to the airway; and the need for maintaining in-line cervical spine stabilization are common conditions that can complicate airway management in trauma.
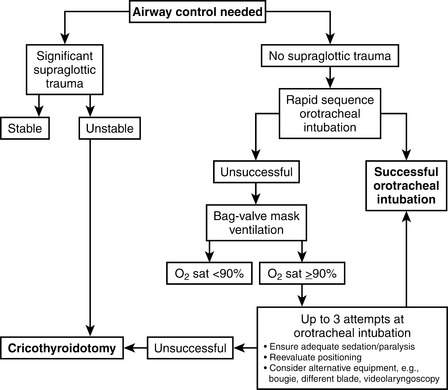
All trauma care providers should have experience with airway evaluation and management from manual airway maneuvers (e.g., jaw thrust, chin lift), to the use of mechanical airway devices (oropharyngeal and nasopharyngeal airways), to bag-mask ventilation, to rapid-sequence endotracheal intubation, to the use of airway adjuncts such as the bougie or laryngeal mask airway, to establishing a surgical airway. A general algorithm for trauma airway management is shown in Figure 2-1.
6 What is the role of the FAST examination in evaluating the trauma patient with hemodynamic instability?
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


