Gastrointestinal Bleeding
KEY POINTS
1 Prophylactic treatments can reduce the incidence of upper gastrointestinal bleeding in patients at high risk (e.g., chronic mechanical ventilation, coagulation disorders). Prophylactic methods include acid suppression or neutralization or gastric mucosal coating. The best prophylaxis is maintenance of good splanchnic perfusion and provision of enteral feeding as early as tolerated.
2 Upper gastrointestinal bleeds are usually readily distinguished from lower tract bleeds by simple history and physical examination. Vomiting blood is a highly reliable sign of upper gastrointestinal bleeding, whereas hematochezia may result from an upper or lower source. Melena is highly suggestive of an upper bleeding source.
3 With the possible exception of varices and ulcers containing visible vessels or overlying clots, most gastrointestinal bleeding ceases spontaneously; hence, therapy is supportive.
4 Esophagogastroduodenoscopy provides a rapid, safe, and precise method to diagnose the source of upper gastrointestinal bleeding, offers several therapeutic options (injection therapy, thermal coagulation), and provides useful prognostic information.
5 Significant lower gastrointestinal bleeding is less common than bleeding from an upper source. If the bowel can be evacuated, colonoscopy provides a diagnosis in most cases. With briskly bleeding lower gastrointestinal lesions, angiography or nuclear scans offer alternative diagnostic options.
▪ PREVENTION
In decades past the development of upper gastrointestinal (UGI) bleeding from diffuse “stress ulceration” complicated the stay of up to 30% of critically ill patients. Fortunately, the incidence of significant UGI bleeding developing in the ICU has declined dramatically. Although this is partly the result of the widespread use of histamine (H2) blockers, proton pump inhibitors (PPIs) and other gastroprotective agents, many other practices have also changed. For example, it is much more common to use mucosal protective enteral nutrition earlier and instead of total parenteral nutrition (TPN). Use of ulcerogenic medications including corticosteroids, slow-release potassium tablets, and oral nonsteroidal anti-inflammatory agents is also less common. Because shock is a potent risk factor for mucosal ulceration and mesenteric ischemia, it is also likely that more aggressive resuscitation practices are partly responsible for the reduced risk of bleeding. Finally, sedation, ventilation, and weaning protocols have shortened the time on ventilator reducing the period of risk.
Indications
Not all ICU patients require pharmacologic “ulcer prophylaxis”; however, prevention efforts are indicated for patients undergoing prolonged (>48 h) mechanical ventilation, for patients with coagulation disorders (e.g., thrombocytopenia, consumptive, hereditary, or anticoagulation related), and for patients with renal failure. Other reasonable candidates include patients with burns, trauma, head injury, and those receiving corticosteroids. As the number of risk factors mounts, so should the likelihood to prescribe prophylaxis. For patients receiving enteral nutrition, prophylaxis may add cost without potential benefit, especially for nonventilated patients.
Options
If mucosal protection or pharmacologic gastric acid buffering is deemed necessary, H2 blockers, PPIs, sucralfate, and antacids are available to accomplish the task. Although controversial, no convincing data suggest the superiority of one class of agent over another or the superiority of any specific drug within a class. Hence, drug selection should be based on side effect profile, cost, and convenience. Clinical practice is heterogeneous but currently PPIs are the most widely used drugs.
Antacids are inconvenient because they must be administered every 1 to 2 h, interact with other enteral medications, and often cause diarrhea, phosphate binding, and (in renal insufficiency) the potential for magnesium toxicity. Obviously, antacids cannot deter gastric ulceration if introduced through a postpyloric feeding tube. Antacids are also associated with the highest incidence of reflux and surprisingly may be the most expensive choice.
Because sucralfate requires acid for dissolution and tissue binding, it is ineffective if administered with antacids, H2 blockers, or PPIs, and is less effective and perhaps unnecessary if given with enteral feeding. Sucralfate is problematic because it reduces bioavailability of several commonly used drugs (e.g., quinolones, phenytoin, tetracycline, warfarin, and fluconazole). A commercially available liquid preparation avoids the inconvenience of pulverizing tablets, suspending them in solution and forcing the solution through an enteral tube (often clogging it).
Because the efficacy of continuous intravenous (IV) infusions, intermittent injections, and oral dosing of all available H2-blocking appear equivalent, it is reasonable to use the least-expensive oral agent. Significant side effects of H2 blockers are rare but include altered drug metabolism and confusion (most frequently reported with cimetidine). Although often discussed, there is little evidence that H2 blockers are associated with development of thrombocytopenia.
By inhibiting the final step in acid secretion, PPIs given once or twice daily effectively raise gastric pH to a greater degree and for longer periods than H2 blockers. Despite this observation there are no credible data to suggest that PPIs given either IV or enterally are superior to H2 blockers for the primary prevention of UGI bleeding. Some PPIs (e.g., lansoprazole, omeprazole) are supplied as capsules containing entericcoated granules, which must be suspended in a pH buffering liquid if administered by tube. Like sucralfate, these preparations often clog small-bore tubes. As a group, PPIs are very safe but their use increases the absorption of digoxin, calcium channel blockers, benzodiazepines, and opiates. The clinical importance of rebound acid hypersecretion is uncertain but occurs commonly with discontinuation of PPIs.
Risks
Although debated, gastric acid suppression, regardless of how it is achieved, is probably associated with a small increase in risk of nosocomial pneumonia. The mechanism is believed to be the result of gastric overgrowth of microorganisms with subsequent aspiration. Not only does gastric pH play a role, stomach volume and patient position do as well. This is evidenced by the finding that pneumonia risk is comparable when using H2 blockers, PPIs, or sucralfate but higher when using large volumes of antacids. Regardless, the balance favors bleeding prophylaxis. When prophylaxis is used, effective measures to lower the risk of pneumonia are to elevate the head of the bed to at least 30 degree for all patients who can tolerate such positioning; avoid bolus enteral feedings; and provide consistent oral hygiene. Doing so reduces the reflux of gastric contents and the potential for aspiration and lowers the burden of pathogenic organisms that may be aspirated.
▪ EVALUATION OF THE BLEEDING PATIENT
First steps
In patients with conspicuous GI bleeding, attention should first be devoted to ensuring a stable airway with adequate ventilation and establishing intravenous access. Developing an appropriate and efficient diagnostic and therapeutic plan requires distinguishing upper from lower bleeding using historical and demographic information and the examination. UGI bleeding is more likely among younger patients and men. A history of repeated retching, non-steroidal anti-inflammatory drug (NSAID) use, heavy alcohol ingestion, or past history of peptic ulcer disease or liver disease (especially with varices) favors an UGI bleeding source. By contrast, lower GI (LGI) bleeding is more likely among older patients, women, and patients with a history of diverticular or vascular occlusive disease. GI bleeding occurring during systemic anticoagulation does not preferentially occur from an upper or lower source.
Examination
Bruising or petechiae may be a clue to an underlying coagulopathy, and cutaneous or mucous membrane arteriovenous malformations may signal the presence of hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome). Mental status alterations can result from hypotension alone but often indicate the presence of hepatic encephalopathy. The stigmata of cirrhosis and portal hypertension (e.g., jaundice, ascites, spider angiomata, caput medusa, palmar erythema, gynecomastia, ecchymoses) make a diagnosis of UGI bleeding much more likely.
The predominant portal of blood loss (oral or rectal) provides a valuable guide to bleeding site. Hematemesis is rarely the result of LGI bleeding and essentially never results from a source beyond the proximal jejunum. By contrast, hematochezia can result from brisk upper or slower LGI bleeding, but in the absence of shock is almost always due to a LGI source. As little as 15 mL of blood in the UGI tract may produce guaiac-positive stools, but melena (black, tarry stools formed by the digestion of blood by acid and bacteria) requires loss of more than 100 mL of blood over a relatively brief period. Because blood in the gut speeds transit time, melena seldom results from LGI bleeding unless it originates from a slow bleed in the ascending colon. More commonly, significant bleeding from the right colon produces maroon-colored stools, whereas bleeding from the left colon results in hematochezia. A mixture of formed stool with red blood is highly suggestive of a distal colonic (sigmoid colon or rectal) source.
An UGI bleed is less likely if the aspirate from a gastric tube does not reveal fresh blood or at least “coffee ground” material, although as many as 15% of patients with UGI bleeding have clear aspirates. These “false-negative” aspirates usually occur when a competent pylorus prevents reflux of blood originating in the duodenum into the stomach. Testing gastric contents is not warranted because it commonly produces false-positive results.
Assessing Bleeding Severity
For the average sized adult, blood loss of less than 1 L produces few physiological changes as pulse, respiratory rate, blood pressure, mental status, and urine output remain near normal. With acute losses of 1 to 1.5 L (mild shock) tachycardia, tachypnea, and mild oliguria are seen and orthostatic blood pressure changes can be detected. Tachypnea can be an appropriate compensatory response to hemorrhage and metabolic acidosis, the result of aspirating vomited blood, or only a manifestation of anxiety. Moderate shock following hemorrhage of 1.5 to 2 L raises pulse and respiratory rates further, causes confusion, slows capillary refill, and further diminishes urine output. When severe shock occurs, typically with blood losses more than 2 L hypotension is routine and profound, tachycardia marked, and enormous ventilatory demands often cause respiratory collapse. Urine output and mental status are never normal. During acute hemorrhage it is important to not be misled by hemoglobin (Hgb) measurements. In severe acute blood loss, the Hgb concentration remains near normal despite massive losses until crystalloid replacement is begun. By contrast, a very low Hgb concentration in a patient with near normal vital signs almost certainly means blood loss has occurred over weeks or even months. Hence, shock with visible loss of large volumes of blood should prompt aggressive transfusion, whereas severe anemia without visible evidence of blood or shock can be approached more slowly.
Initial Treatment
As stabilization is accomplished appropriate consultants (e.g., gastroenterology, interventional radiology, surgery) should be notified. For patients with shock, massive hematemesis, or incipient respiratory failure, it usually makes sense to perform endotracheal intubation before overwhelming aspiration or respiratory arrest occur. In addition, upper endoscopic evaluation is often not possible without airway control. Caution is advised however; frequently, the procedure prompts massive hematemesis obscuring the airway. Powerful suction and expert backup are essential. When time permits, evacuation of the stomach with a gastric tube may reduce regurgitation risk. Gown, gloves, and face-shield protection for the proceduralist is prudent.
Regardless of bleeding source, at least two large-bore (16- to 14-gauge) peripheral IV catheters or a large central venous catheter (CVC) should be inserted to allow rapid fluid and blood administration. A CVC is not always necessary and may not be the best choice for fluid infusion, but the central venous pressure (CVP) measurements it yields can be useful to guide fluid replacement. (A triple-lumen catheter may actually slow fluid administration because its three smaller lumens and increased length cannot achieve the same infusion rates as shorter, larger bore peripheral IVs.) By contrast, a centrally placed 7.5- or 8.5-F conduit can deliver prodigious amounts of fluid and blood, especially if used with a pressure infuser.
At the time IV access is obtained, samples should be obtained for Hgb, electrolytes, creatinine, liver function tests, prothrombin time (PT), platelet count, and cross-matching. Arterial blood gas testing may be useful to evaluate adequacy of ventilation and severity of metabolic acidosis. The basic principles of support of the circulation and transfusion are presented in Chapters 3 and 14, respectively;
however, a few points deserve emphasis. First, the fundamental problem in severe GI bleeding is intravascular volume depletion. Therefore, the best first therapy is not vasopressor infusion but isotonic crystalloid replacement followed by blood when available. Colloid offers no demonstrated advantage over crystalloid resuscitation, despite the fact that a smaller volume of the former is required to produce equivalent volume expansion. Colloids risk allergic reaction, are not always immediately available, and are more than ten times more expensive than crystalloid for equal effect. Although fresh whole blood is a better source of oxygen delivery than older packed red blood cells, it is rarely available. As a consequence, blood replacement is usually accomplished using specific component therapy with serial assessments of Hgb, platelet count, and PT. For exsanguinuating patients, universal donor (O negative) blood may be necessary, but if there are even a few minutes to spare, the possibly safer alternative is type-specific red blood cells. Thrombocytopenia or soluble clotting factor deficiencies should be corrected rapidly to promote hemostasis. Prevention or reversal of hypothermia and metabolic acidosis are additional methods of optimizing coagulation. Reasonable transfusion goals are ≥50,000/mm3 functioning platelets, a PT less than 1.5 times control, and a Hgb more than 8 gm/dL. Although it is clear that lower transfusion thresholds are safe for the nonbleeding patient, during ongoing hemorrhage it is prudent to maintain a buffer against exsanguination. Even higher Hgb values may be appropriate in patients with critical oxygen supply problems, such as recent myocardial ischemia or stroke.
however, a few points deserve emphasis. First, the fundamental problem in severe GI bleeding is intravascular volume depletion. Therefore, the best first therapy is not vasopressor infusion but isotonic crystalloid replacement followed by blood when available. Colloid offers no demonstrated advantage over crystalloid resuscitation, despite the fact that a smaller volume of the former is required to produce equivalent volume expansion. Colloids risk allergic reaction, are not always immediately available, and are more than ten times more expensive than crystalloid for equal effect. Although fresh whole blood is a better source of oxygen delivery than older packed red blood cells, it is rarely available. As a consequence, blood replacement is usually accomplished using specific component therapy with serial assessments of Hgb, platelet count, and PT. For exsanguinuating patients, universal donor (O negative) blood may be necessary, but if there are even a few minutes to spare, the possibly safer alternative is type-specific red blood cells. Thrombocytopenia or soluble clotting factor deficiencies should be corrected rapidly to promote hemostasis. Prevention or reversal of hypothermia and metabolic acidosis are additional methods of optimizing coagulation. Reasonable transfusion goals are ≥50,000/mm3 functioning platelets, a PT less than 1.5 times control, and a Hgb more than 8 gm/dL. Although it is clear that lower transfusion thresholds are safe for the nonbleeding patient, during ongoing hemorrhage it is prudent to maintain a buffer against exsanguination. Even higher Hgb values may be appropriate in patients with critical oxygen supply problems, such as recent myocardial ischemia or stroke.
For most patients with UGI bleeding, gentle placement of a nasogastric (NG) or orogastric (OG) tube is safe and useful to monitor the rate of bleeding. Although controversial, possible exceptions include patients with esophageal varices or Mallory -Weiss tears in whom tube placement theoretically could aggravate bleeding. Combining clinical data with gastric aspirate results also has prognostic value. Clear or “coffee ground” returns portend a good prognosis when the patient presents with melena. When red blood is aspirated from the stomach of a patient with melena, the prognosis is worse but not as bad as when red blood is recovered from the stomach during hematochezia. Patients with liver failure may benefit from purging intestinal blood that can precipitate hepatic encephalopathy, but blood is an excellent laxative, usually making cathartics unnecessary. Gastric lavage does not decrease the rate of UGI bleeding, even when the solution is cooled or fortified with vasoconstrictor.
▪ UGI BLEEDING
Sources
A relatively small number of conditions are responsible for most cases of UGI bleeding (Table 37-1). Peptic ulcer disease (gastric and duodenal ulcer) leads the list, followed by gastric and esophageal erosive disease, Mallory-Weiss tears, and variceal bleeding. Making a definitive diagnosis of an UGI bleeding source usually is straightforward and is outlined in Figure 37-1. Fortunately, regardless of cause, UGI bleeding stops spontaneously in 70% to 80% patients. A combination of clinical factors (i.e., older age, shock at presentation, coagulopathy, or renal, hepatic, or heart failure) and specific endoscopic findings (Table 37-2) predict those most likely to have recurrent bleeding.
Diagnostic Tests
Plain abdominal radiographs are rarely diagnostically useful unless they demonstrate free air (indicating perforation of a viscus) or “thumbprinting” of the large bowel (suggesting ischemic colitis). Likewise, the long used “UGI series” is seldom diagnostic and swallowed barium compromises subsequent tests, including endoscopy, CT scanning, and angiography and makes surgery technically more difficult. Barium studies also require transport of potentially unstable patients to the radiography suite.
Esophagogastroduodenoscopy (EGD) is a highyield procedure to (a) definitively demonstrate the
bleeding site, (b) predict the likelihood for rebleeding, (c) permit control of some lesions, and (d) reduce resource utilization (e.g., transfusions, operating room time if surgery is required, and hospital length of stay). However, EGD has several limitations: sedation may compromise ventilation in tenuous patients, and an optimal examination requires a stomach empty of food and blood. (A single 250-mg dose of IV erythromycin given 30 min before endoscopy can increase gastric emptying and improve visualization.)
bleeding site, (b) predict the likelihood for rebleeding, (c) permit control of some lesions, and (d) reduce resource utilization (e.g., transfusions, operating room time if surgery is required, and hospital length of stay). However, EGD has several limitations: sedation may compromise ventilation in tenuous patients, and an optimal examination requires a stomach empty of food and blood. (A single 250-mg dose of IV erythromycin given 30 min before endoscopy can increase gastric emptying and improve visualization.)
TABLE 37-1 SOURCES OF UGI BLEEDING | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
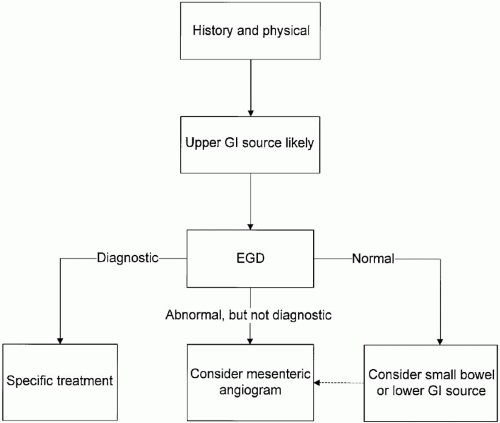 ▪ FIGURE 37-1 Suggested diagnostic evaluation of suspected upper GI bleeding. If upper GI bleeding is believed to be likely after obtaining a history and performing a physical examination, esophagogastroduodenoscopy (EGD) is usually performed. If EGD is diagnostic, therapy directed at the specific lesion should be instituted. If the EGD is normal, the small bowel or LGI tract should be considered as a bleeding source. When the EGD is abnormal but nondiagnostic, consideration should be given to mesenteric angiography. |
The best time to perform EGD is debated but is probably as soon as the airway and oxygenation are adequate and a reasonable degree of hemodynamic stability is achieved. Based on the combination of clinical and endoscopic features, it is undoubtedly safe to provide care outside the ICU and even discharge patients with lesions at low risk to rebleed (i.e., gastritis, clean-based ulcers, or flat pigmented spots). By contrast, patients with bleeding varices and those with ulcers containing visible vessels or obscured by overlying clot are at high risk for recurring hemorrhage.
TABLE 37-2 RISK OF RECURRENT UPPER GI BLEEDING BASED ON ENDOSCOPIC FINDINGS | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


