CHAPTER 30
Foreign Body, Throat
Presentation
The patient is usually convinced that there is a foreign body (FB) stuck in his throat, because he recently swallowed something, such as a fish or chicken bone, and can still feel a “sensation” in the throat, especially (perhaps painfully) when swallowing. He may be able to localize the FB sensation to precisely above the thyroid cartilage (which implies an FB in the hypopharynx that may be visible), or he may only vaguely localize the FB sensation to the suprasternal notch (which could imply an FB anywhere in the esophagus).
Those with dentures, especially full dentures, are more likely to swallow a bone because of reduced sensitivity and inability to chew properly. Fish bones, which are usually long, are commonly caught in the oropharynx, particularly at the region of the tonsils and the tonsillar pillars. At these regions, fish bones can usually be grasped and extracted, as long as they can be visualized.
An FB lodged in the tracheobronchial tree usually stimulates coughing and wheezing. Obstruction of the esophagus produces drooling and causes the patient to spit up whatever fluid is swallowed. Any infant who refuses to eat or who has trouble handling buccal secretions should be evaluated for an FB.
What To Do:
 FBs in the throat can lead to partial or complete airway obstruction. If complete or near-complete obstruction is present, immediate intervention with direct visualization using a laryngoscope and removal with an instrument, such as a McGill forceps, is indicated.
FBs in the throat can lead to partial or complete airway obstruction. If complete or near-complete obstruction is present, immediate intervention with direct visualization using a laryngoscope and removal with an instrument, such as a McGill forceps, is indicated.
 If the patient can cough and verbalize and is not in significant distress, but appears to have a partial airway obstruction, it is better to place him in the most comfortable position, provide supplemental oxygen, and call in a multidisciplinary team, including an ear-nose-throat (ENT) specialist and anesthesiologist, to perform removal in the operating room.
If the patient can cough and verbalize and is not in significant distress, but appears to have a partial airway obstruction, it is better to place him in the most comfortable position, provide supplemental oxygen, and call in a multidisciplinary team, including an ear-nose-throat (ENT) specialist and anesthesiologist, to perform removal in the operating room.
 If the patient has no evidence of airway obstruction, but only the sensation of an FB in the throat, establish exactly what was swallowed, when, and the progression of symptoms. Patients can accurately tell if an FB is on the right or left side.
If the patient has no evidence of airway obstruction, but only the sensation of an FB in the throat, establish exactly what was swallowed, when, and the progression of symptoms. Patients can accurately tell if an FB is on the right or left side.
 Examine the anterior neck for tenderness, masses, or subcutaneous emphysema (suggests perforation). Percuss and ascultate the chest. An FB sensation in the throat can be produced by a pneumothorax, pneumomediastinum, or esophageal disease, all of which may show up on a chest radiograph.
Examine the anterior neck for tenderness, masses, or subcutaneous emphysema (suggests perforation). Percuss and ascultate the chest. An FB sensation in the throat can be produced by a pneumothorax, pneumomediastinum, or esophageal disease, all of which may show up on a chest radiograph.
 Inspect the hypopharynx using a good light or headlamp mirror and tongue depressor, paying special attention to the base of the tongue, tonsils, and vallecula, where foreign bodies are likely to lodge. Place the tongue depressor at the middle third of the tongue and press firmly downward to give good exposure without making the patient gag. You can also maximize visibility and exposure, without making the patient gag, by holding the tongue out (use a washcloth or 4 × 4-inch gauze for traction), taking care not to lacerate the frenulum of the tongue on the lower incisors, and then instruct the patient to raise his soft palate by “panting like a dog.”
Inspect the hypopharynx using a good light or headlamp mirror and tongue depressor, paying special attention to the base of the tongue, tonsils, and vallecula, where foreign bodies are likely to lodge. Place the tongue depressor at the middle third of the tongue and press firmly downward to give good exposure without making the patient gag. You can also maximize visibility and exposure, without making the patient gag, by holding the tongue out (use a washcloth or 4 × 4-inch gauze for traction), taking care not to lacerate the frenulum of the tongue on the lower incisors, and then instruct the patient to raise his soft palate by “panting like a dog.”
 This may be accomplished without topical anesthesia, but if the patient tends to gag, the soft palate and posterior pharynx can be anesthetized by spraying with Cetacaine, Hurricaine, or 10% lidocaine, or by having the patient gargle with lidocaine (viscous Xylocaine) diluted 1:1 with water. Some patients may continue to gag even with the topical anesthesia.
This may be accomplished without topical anesthesia, but if the patient tends to gag, the soft palate and posterior pharynx can be anesthetized by spraying with Cetacaine, Hurricaine, or 10% lidocaine, or by having the patient gargle with lidocaine (viscous Xylocaine) diluted 1:1 with water. Some patients may continue to gag even with the topical anesthesia.
 If the object can be seen directly, carefully grasp and remove it with bayonet or curved forceps (Figure 30-1). Objects at the base of the tongue or in the hypopharynx may require a mirror or indirect laryngoscope for visualization. Small fish bones are frequently difficult to see. They may be overlooked entirely except for their tips, or they may only appear to be threads of mucus, Fiberoptic nasopharyngoscopy, usually performed by an ENT specialist, is preferred, when available.
If the object can be seen directly, carefully grasp and remove it with bayonet or curved forceps (Figure 30-1). Objects at the base of the tongue or in the hypopharynx may require a mirror or indirect laryngoscope for visualization. Small fish bones are frequently difficult to see. They may be overlooked entirely except for their tips, or they may only appear to be threads of mucus, Fiberoptic nasopharyngoscopy, usually performed by an ENT specialist, is preferred, when available.
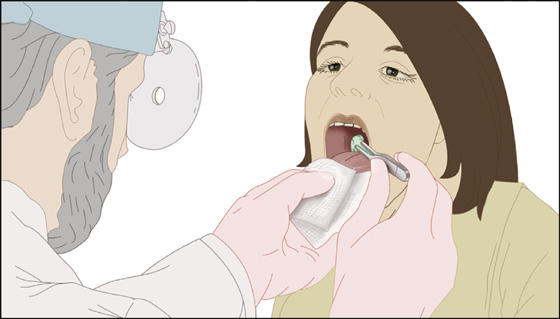
Figure 30-1 Carefully grasp and remove any foreign body that can be seen in the throat.
 If the symptoms are mild and a foreign body cannot be visualized, test the patient’s ability to swallow, first using a small cup of water and then a small piece of soft bread. If the patient can swallow liquids and solids, they may be safely discharged. They should be instructed to seek follow-up care as soon as possible if the pain worsens, fever develops, or if breathing or swallowing is difficult. They should be seen by an ENT specialist or return to the ED or clinic if they are not better in 2 days.
If the symptoms are mild and a foreign body cannot be visualized, test the patient’s ability to swallow, first using a small cup of water and then a small piece of soft bread. If the patient can swallow liquids and solids, they may be safely discharged. They should be instructed to seek follow-up care as soon as possible if the pain worsens, fever develops, or if breathing or swallowing is difficult. They should be seen by an ENT specialist or return to the ED or clinic if they are not better in 2 days.
 If the pain or FB sensation is moderate to severe, or if there is bleeding or fever, and the FB cannot be visualized, CT scanning is the test of choice to diagnose FBs that may not be easily seen on plain radiography.
If the pain or FB sensation is moderate to severe, or if there is bleeding or fever, and the FB cannot be visualized, CT scanning is the test of choice to diagnose FBs that may not be easily seen on plain radiography.
 If an FB is discovered on CT, but cannot be visualized on physical examination, obtain an ENT consultation. Consider an ENT consultation even if the CT is negative and you are still very suspicious of an FB, because CT scanning is associated with a small percentage of false-negative examinations.
If an FB is discovered on CT, but cannot be visualized on physical examination, obtain an ENT consultation. Consider an ENT consultation even if the CT is negative and you are still very suspicious of an FB, because CT scanning is associated with a small percentage of false-negative examinations.
 If the ENT evaluation of the hypopharynx is negative and the pain is persistent, (especially pain localized to the suprasternal notch), consider that the FB may be in the esophagus and consult a gastroenterologist.
If the ENT evaluation of the hypopharynx is negative and the pain is persistent, (especially pain localized to the suprasternal notch), consider that the FB may be in the esophagus and consult a gastroenterologist.
 An impacted button battery represents a true emergency and requires rapid removal, because leaking alkali produces liquefactive necrosis. Button batteries of all sizes have a distinctive double contour on radiography.
An impacted button battery represents a true emergency and requires rapid removal, because leaking alkali produces liquefactive necrosis. Button batteries of all sizes have a distinctive double contour on radiography.
 A tablet composed of irritating medicine, if swallowed without adequate liquid, may stick to the mucosa of the pharynx or esophagus and cause an irritating ulcer with a foreign body sensation.
A tablet composed of irritating medicine, if swallowed without adequate liquid, may stick to the mucosa of the pharynx or esophagus and cause an irritating ulcer with a foreign body sensation.
 When coughing or wheezing suggests aspiration of an FB into the tracheobronchial tree, a chest radiograph with expiratory views should be obtained. If these are negative, a chest CT scan should be performed. If a foreign body is found in the pulmonary tree, a pulmonary specialist consultation should be obtained.
When coughing or wheezing suggests aspiration of an FB into the tracheobronchial tree, a chest radiograph with expiratory views should be obtained. If these are negative, a chest CT scan should be performed. If a foreign body is found in the pulmonary tree, a pulmonary specialist consultation should be obtained.
 If CT studies are normal, careful inspection does not reveal an FB, and the patient is afebrile with only mild discomfort, he may be sent home. Reassure him that a scratch on the mucosa can produce a sensation that the FB is still there. Also inform him that if the symptoms worsen or fail to resolve in 2 days, he may need further endoscopic studies to look for a hidden problem.
If CT studies are normal, careful inspection does not reveal an FB, and the patient is afebrile with only mild discomfort, he may be sent home. Reassure him that a scratch on the mucosa can produce a sensation that the FB is still there. Also inform him that if the symptoms worsen or fail to resolve in 2 days, he may need further endoscopic studies to look for a hidden problem.
What Not To Do:
 Do not assume that a foreign body is absent just because the pain disappears after a local anesthetic is applied.
Do not assume that a foreign body is absent just because the pain disappears after a local anesthetic is applied.
 Do not order plain radiographs or a barium swallow to evaluate suspected fish bone impactions. The results are unreliable or misleading, and with barium, subsequent examinations of a coated esophagus are made more difficult.
Do not order plain radiographs or a barium swallow to evaluate suspected fish bone impactions. The results are unreliable or misleading, and with barium, subsequent examinations of a coated esophagus are made more difficult.
 Do not attempt to remove a strand of mucus that mimics the appearance of a delicate fish bone; when you grab it and it behaves like a thread of mucus, it is a thread of mucus.
Do not attempt to remove a strand of mucus that mimics the appearance of a delicate fish bone; when you grab it and it behaves like a thread of mucus, it is a thread of mucus.
 Do not reassure the patient that the presence of a foreign body has been ruled out if it has not been completely ruled out. Explain that although you think there is a low probability that a foreign body exists, careful follow-up needs to be obtained if symptoms do not resolve.
Do not reassure the patient that the presence of a foreign body has been ruled out if it has not been completely ruled out. Explain that although you think there is a low probability that a foreign body exists, careful follow-up needs to be obtained if symptoms do not resolve.
 Do not overlook the possibility of preexisting pathologic conditions discovered incidentally during swallowing.
Do not overlook the possibility of preexisting pathologic conditions discovered incidentally during swallowing.
 Do not attempt to remove a foreign body from the throat blindly by using a finger or instrument, because the object may be pushed farther down into the airway and obstruct it or may cause damage to surrounding structures.
Do not attempt to remove a foreign body from the throat blindly by using a finger or instrument, because the object may be pushed farther down into the airway and obstruct it or may cause damage to surrounding structures.
Most of these patients have a sharp pricking-pain sensation on swallowing, but no specific sign or symptom will consistently rule in or rule out a retained bone.
During swallowing, as the base of the tongue pushes a bolus of food posteriorly, any sharp object hidden in that bolus may become embedded in the tonsil, the tonsillar pillar, the pharyngeal wall, or the tongue base itself. Symptomatic patients are convinced that they have a bone stuck in the throat, although in most patients no bone is found and the symptoms resolve spontaneously. In two studies, approximately 25% of the patients with symptoms of an embedded fish bone had no demonstrable pathologic findings, and their symptoms resolved in 48 hours. Only 20% actually had an embedded fish bone, and most of these were easily identified and removed on the initial visit.
All patients who complain of a foreign body in the throat should be taken seriously. Even relatively smooth or rounded objects that remain impacted in the esophagus have the potential to cause serious problems. A fish bone can perforate the esophagus in only a few days, and chicken bones carry even greater risk for serious injuries, such as a neck abscess, mediastinitis, and an esophageal carotid artery fistula.
The sensation of a lump in the throat, unrelated to swallowing food or drink, may be globus hystericus, which is related to cricopharyngeal spasm and anxiety. The initial workup is the same as that for any foreign body sensation in the throat.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


