Critical Care Medicine
Adult Critical Care
CPAP for acute cardiogenic pulmonary oedema from out-of-hospital to cardiac intensive care unit: a randomised multicentre study
Ducros L, on behalf of the CPAP collaborative study group (Hôpital Universitaire Lariboisiére, Paris, France; et al) Intensive Care Med 37:1501-1509, 2011§
Evidence Ranking
• A
Expert Rating
• 3
Abstract
Conclusion
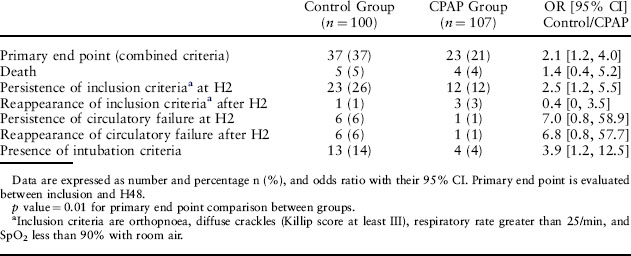
Immediate use of CPAP in out-of-hospital treatment of CPE and until CPE resolves after admission significantly improves early outcome compared with medical treatment alone (Tables 2–4).
Table 2 Physiological Parameters at Study Entry and Echocardiographic Findings
| Parameters | Control Group (N = 100) | CPAP Group (N = 107) |
|---|---|---|
| SpO2 in air (%) | 84 [78, 88] | 84 [80, 88] |
| pH | 7.30 [7.22, 7.36] | 7.30 [7.25, 7.37] |
| PO2 (mmHg) | 127 [86, 177] | 114 [79, 183] |
| PCO2 (mmHg) | 49 [41, 57] | 46 [39, 55] |
| Bicarbonates (mmol/L) | 23 [20, 26] | 24 [20, 26] |
| Respiratory rate (per min) | 35 [30, 40] | 36 [30, 40] |
| Systolic arterial blood pressure (mmHg) | 170 [143, 193] | 170 [150, 195] |
| Diastolic arterial blood pressure (mmHg) | 97 [80, 103] | 95 [82, 110] |
| Heart rate (bpm) | 101 [90, 116] | 102 [83, 116] |
| Encephalopathy | 7 (7) | 13 (12) |
| Circulatory failure | 18 (18) | 17 (16) |
| Echocardiographic findings LVEF | 35 [30, 60] | 45 [35, 60] |
| Syst. PAP (mmHg) | 40 [32, 45] | 38 [31, 43] |
| E/A ratio | 0.9 [1, 1] | 0.9 [1, 2] |
Data are expressed as median with 25th and 75th interquartile range [Q1, Q3] or number and percentage n (%); SpO2 pulse oximetry; arterial blood gases were sampled under O2 mask with a reservoir at 15 L/min. LVEF left ventricular ejection fraction, Syst PAP systolic pulmonary arterial pressure (mmHg); E/A ratio flow velocity ratio across the mitral valve between early diastole and atrial contraction.
Related posts:
 of change in daily step count over five years with insulin sensitivity and adiposity: population based cohort study
of Cancer: The Next Generation
Beverages and Risk of Metabolic Syndrome and Type 2 Diabetes: A meta-analysis
time and haemodynamic response after thiopental vs. propofol in the elderly: a randomized trial
monitoring of neuromuscular block over the orbicularis oris muscle in anesthetized patients receiving vecuronium
Is Better Than General Anesthesia During Endovascular Acute Stroke Interventions
of change in daily step count over five years with insulin sensitivity and adiposity: population based cohort study
of Cancer: The Next Generation
Beverages and Risk of Metabolic Syndrome and Type 2 Diabetes: A meta-analysis
time and haemodynamic response after thiopental vs. propofol in the elderly: a randomized trial
monitoring of neuromuscular block over the orbicularis oris muscle in anesthetized patients receiving vecuronium
Is Better Than General Anesthesia During Endovascular Acute Stroke Interventions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


