FIGURE 58.1 Initial management of suspected or confirmed intra-abdominal infections. (Adapted from IDSA–Complicated Intra-abdominal Infection—In Adults. http://www.idsociety.org.)
The clinical presentation of an intra-abdominal abscess often requires a high index of suspicion, as the clinical presentation can be subtle. Nonspecific manifestations including leukocytosis, fever, dysuria or urinary retention, unexplained pleural effusion, and change in bowel function (diarrhea) should alert the physician to investigate for an intra-abdominal infection. Investigation should include a CT scan of the abdomen and pelvis with oral and intravenous contrast. Once an abscess is identified, early antibiotic coverage and source control with either surgical or percutaneous drainage are mandated. Clinical factors predicting the failure of source control for intra-abdominal infections are outlined in Table 58.1 (4).
The microbiology of abscesses is dependent on the organ involved and duration of critical illness. Figure 58.2 outlines the antibiotic management guidelines of patients with community-acquired intra-abdominal infections (4). The stomach and duodenum normally have sparse bacterial colonization due to the acid concentration in these segments. The flora is mainly composed of swallowed oral organisms such as microaerophilic streptococci and Streptococcus viridans, lactobacillus, fusiform bacteria, and Candida. The concentration of organisms may be altered and significantly increased in patients with acid-suppressive treatment, gastric obstruction, and achlorhydria. The concentration of small bowel flora is variable throughout its length, with greater concentration distally. The normal flora consists primarily of the Enterobacteriaceae, Enterococcus, and anaerobic species. The colon contains a combination of both aerobic and anaerobic bacteria with anaerobes constituting 90% of the bacterial load. Aerobic bacteria are primarily gram-negative rods consisting of the Enterobacteriaceae (Escherichia coli, Klebsiella spp., Enterobacter spp., and Proteus spp.), Pseudomonas, and gram-positive Enterococci. Anaerobic bacteria include Bacteroides fragilis, Bacteroides subspecies, Clostridium spp., Eubacterium spp., and Bifidobacterium spp.; intra-abdominal abscesses are typically polymicrobial.
| TABLE 58.1 Clinical Factors Predicting Failure of Source Control for Intra-abdominal Infection |
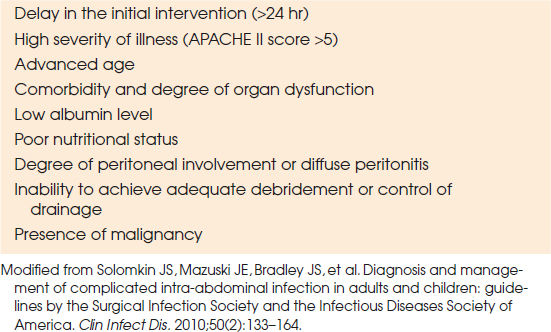 |

FIGURE 58.2 Microbiology and management of community-acquired intra-abdominal infections in adults. (Adapted from IDSA–Complicated Intra-abdominal Infection—In Adults. http://www.idsociety.org.)
Patients with generalized peritonitis or hemodynamic instability with suspected intra-abdominal infection require emergent surgical exploration to identify the cause. The primary source of the infection is controlled by repair or resection followed by a thorough washout of the abdominal cavity with warm saline. In some patients with either hemodynamic instability or severe contamination, the abdominal wall may be temporarily left open for additional washout in 24 to 48 hours. Management of the open abdomen is discussed later.
Stable patients with localized peritonitis or suspected intra-abdominal sepsis should undergo a CT scan to identify any abnormal pathology; if a defined abscess or fluid collection is seen on the CT scan, percutaneous drainage is possible using CT or ultrasound image guidance. This technique is well established (5–7) and minimally invasive; re-exploration of the abdomen may be fraught with difficulty (8).
Antibiotic therapy is based on empiric coverage of bacteria normally present within the gut. Antibiotic coverage should include gram-positive, gram-negative, and anaerobic bacteria; therapy can be focused when culture and sensitivities testing is complete. However, due to problems with anaerobic culturing and identification, most patients should receive anaerobic coverage for gut-associated infection, even when anaerobes are not identified. Antifungal agents are not given even if fungi are seen on cultures, unless the patient is immunosuppressed or has recurrent intra-abdominal infection. Guidelines are published elsewhere (4).
Mortality from intra-abdominal sepsis depends on severity and ranges from 7.5% to 43% (9). Mortality correlates with acute physiology score, malnutrition, age, and shock. Early goal-directed therapy targeted at prompt recognition of abdominal sepsis, broad-spectrum antibiotics, and source control will maximize outcomes.
Pneumoperitoneum
The presence of pneumoperitoneum on x-ray is a finding of a perforated viscous until proven otherwise. The exception is the presence of free air less than 48 hours after laparotomy or laparoscopy; pneumoperitoneum greater than 48 hours postoperation is considered pathologic and requires investigation.
The most common cause of pneumoperitoneum is perforation of the stomach or duodenum from peptic ulcer disease. Free air is also seen in patients with perforation of the colon due to diverticular disease or iatrogenic from endoscopy. Barotrauma to the lung from high-pressure mechanical ventilation can result in pneumoperitoneum (10). The mechanism is thought to be related to the tracking of air from ruptured or distended alveoli toward the mediastinum then dissecting toward the peritoneal cavity. Patients with severe chest trauma resulting in a pneumothorax and pneumomediastinum can also have pneumoperitoneum. Lastly, in females, the peritoneal cavity communicates with the genital tract through the fallopian tubes. Although rare, this provides a potential pathway for communication of air into the peritoneal cavity.
The presence of pneumoperitoneum requires careful evaluation of the patient as not all conditions require operative intervention. In the ICU, a sedated septic patient with no obvious source of sepsis, in the presence of pneumoperitoneum, should nearly always prompt an exploratory laparotomy.
Biliary Disease
Pathology related to the biliary system is common in critically ill patients and is typically associated with either calculous or acalculous cholecystitis. Patients with pre-existing calculous disease may present with acute cholecystitis, cholangitis, or pancreatitis. Clinically patients may present with a positive Murphy sign, fever, and increased WBC; local peritonitis is found in only 24% of patients (11). On further investigation, laboratory findings include leukocytosis, elevated bilirubin (65%), and elevated liver enzymes in less than 50% (12). Ultrasound is the most favorable imaging modality of the biliary system. Ultrasonographic findings of acute cholecystitis include dilated gall bladder, gall bladder wall thickening, the presence of gall stones, and evidence of pericholecystic fluid. Acute acalculous cholecystitis is more commonly associated with critically ill surgical and medical patients in the ICU. The development of acalculous cholecystitis is associated with narcotic use, gastric suctioning, prolonged ileus, prolonged mechanical ventilation, intravenous hyperalimentation, and massive transfusion (12,13). Acalculous cholecystitis in critically ill patients carries a 40% mortality rate (11,14).
Drainage of the biliary tree and antibiotics are the mainstay of treatment. Drainage can be achieved by surgically placed cholecystostomy tube or a percutaneous cholecystostomy tube.
Pseudo-obstruction of the Colon
An ileus of the colon without mechanical obstruction is referred to as pseudo-obstruction or Ogilvie syndrome (15). This condition is typically seen in elderly patients with prolonged immobility, electrolyte imbalance (hyponatremia and hypokalemia), narcotic use, and mechanical ventilation. Other risk factors include multiple trauma, abdominal and pelvic operations, orthopedic operations, and spinal cord injuries (15,16). On physical examination, the abdomen appears distended and tympanic. Abdominal x-ray demonstrates a distend colon. As the colon distends, the wall tension increases leading to local wall ischemia, necrosis, and perforation. The highest risk is when the colon diameter exceeds 12 cm. Mechanical causes of distal obstruction should be ruled out using a contrast enema or colonoscopy.
Management of colonic pseudo-obstruction is based on nonoperative and operative interventions. Initial management should include gastrointestinal decompression with placement of a gastric sump drain and a rectal tube. Correction of electrolysis, minimization of narcotics, and ambulation are further management adjuncts. If there is no improvement with these interventions, neostigmine should be administered to stimulate colonic motility in the absence of distal obstruction (17). Neostigmine is a parasympathomimetic and is given as 1 to 2 mg i.v. Bradycardia is a significant side effect of neostigmine; therefore, patients should be in a monitored location. Neostigmine should be avoided in patients with baseline bradycardia, hypotension, heart block, or bronchospasm. If a patient is unable to take neostigmine, or previous measures are unsuccessful, cautious colonoscopic decompression can be attempted. Colonoscopy can evaluate for mechanical obstruction, provide colonic decompression, and guide placement of a rectal tube. Surgery is offered to patients who fail conservative management, have complications, or impending colonic rupture. Depending on the extent of colonic abnormality, the suggested operation is typically a total abdominal colectomy, in which case an ileostomy with mucus fistula should be performed.
Acute Mesenteric Ischemia
Acute mesenteric ischemia is an uncommon condition and often results in significant morbidity and mortality (70% to 80%) (18,19). The etiology of acute mesenteric ischemia is either from arterial or venous pathology. Arterial causes are classified as nonocclusive mesenteric ischemia and occlusive mesenteric arterial ischemia. Occlusive disease is further classified as acute mesenteric arterial embolism and acute mesenteric arterial thrombosis. Acute mesenteric ischemia can also be caused by mesenteric venous thrombosis (20–22). Early clinical recognition, workup, and intervention are needed to improve outcome (19). Death occurs from MSOF secondary to ischemia (65%), sepsis (25%), pulmonary failure (8%), and stroke (2%) (23).
The classic presentation of acute mesenteric ischemia is a patient’s complaint of pain out of proportion to physical examination findings. Pain is identified in patients 75% to 90% of the time; nausea, vomiting, and abdominal distention are commonly seen. Leukocytosis (WBC count of 20,000 cells/mm3) is seen in less than half of patients. As the degree of bowel ischemia progresses toward gangrene, patients will have a worsening clinical presentation. Peritoneal irritation, leukocytosis, elevated hematocrit, unexplained acidosis, and blood-tinged fluid on peritoneal lavage are all signs of advancing intestinal necrosis (24) and are associated with significant mortality.
Early management should include aggressive fluid resuscitation to maintain adequate blood flow in the mesenteric vessels. Gastric decompression with a nasogastric tube and continuous hemodynamic monitoring is required. Heparinization should be used if immediate surgery is not undertaken.
With improved resolution of modern CT scanners, the diagnosis of acute intestinal ischemia can often be made. Multidetector CT angiography can differentiate occlusive from nonocclusive disease. Despite this, selective arteriography remains the gold standard in the diagnostic and therapeutic approach to acute mesenteric ischemia. Acute occlusion is best treated by immediate surgical management with an embolectomy or aorto-superior mesenteric artery bypass. The bowel should be evaluated for ischemia with nonviable segments resected. Segments with questionable viability should be re-evaluated after allowing time for reperfusion. Although second-look operations are frequently used at 24 to 48 hours to determine the viability of remaining bowel, survival is not necessarily improved by this technique (25).
In patients with nonocclusive mesenteric ischemia, an angiogram will demonstrate mesenteric vasoconstriction. Interpretation of the angiogram may be difficult if the patient is in shock and on vasopressors (26). Traditionally, treatment included the administration of papaverine (30 to 60 mg/hr) through a catheter placed selectively in the superior mesenteric artery (SMA) (27). Papaverine is continued until repeat arteriogram after 24 hours. Currently, however, there is a worldwide shortage of papaverine. Therefore, alternative treatment such as nitroglycerin, combined with verapamil, is becoming more commonly used. The presence of peritoneal signs mandates surgical exploration to assess bowel viability. Antibiotics are indicated because of the high incidence of positive blood cultures resulting from compromised bowel.
The Difficult Postoperative Abdomen
The practice of surgery carries risk of postoperative complications and often difficult therapeutic choices to manage these complications. Intra-abdominal surgery will inevitably result in adhesion formation, which may lead to recurrent episodes of abdominal pain and partial or complete bowel obstruction. Fistulae may result from the natural progression of intra-abdominal pathology or from iatrogenic injury. Abdominal catastrophes may result in abdominal compartment syndrome (ACS) and the risk of temporary abdominal closures and planned ventral hernias. Less commonly seen are complications of radiation enteritis and short bowel syndrome. The following sections will review many of these difficult postoperative issues with descriptions of etiology, diagnosis, and therapeutic approaches.
Adhesions
Intra-abdominal surgery will inevitably result in the unavoidable consequence of adhesions. Adhesion formation is a normal physiologic response in postoperative healing. Formation of adhesive tissue protects an anastomosis and prevents leaks, in addition to assisting in the body’s attempt to isolate intra-abdominal catastrophes. When adhesive bands become too dense, kink, or encompass loops of bowel, they may result in negative consequences such as bowel obstruction and persistent abdominal pain. Intra-abdominal adhesions are the primary cause for postoperative bowel obstruction, accounting for approximately 75% of cases (28).
The majority (94% to 98%) of abdominal adhesions are acquired from either operative therapy or inflammatory processes. The remaining 2% to 6% of adhesions are congenital. In the reoperative abdomen, adhesions are present in 30% to 40% of patients. The most frequent morbidity in those with postoperative adhesions is small bowel obstruction, which accounts for 12% to 17% of hospital admissions following previous abdominal surgery (29). The degree of morbidity related to adhesion formation is related to the type of surgery performed. Laparoscopic surgeries have a 15% adhesion rate as opposed to open laparotomies, in which 50% result in adhesion formation. Adhesions form more commonly following surgery to the small and large bowels and uterus than with other intra-abdominal organs, especially in surgeries involving bowel distal to the transverse colon or involving gynecologic organs (28). The areas most frequently affected are the undersurface of the midline incision and the operative site. The omentum is the most frequently involved organ (57%). Small and large bowel adhesions continue to result in the highest morbidity (30). Adhesions may result in mechanical fixation points where the bowel may kink, wrap around, or become strangulated, thereby compromising enteric flow and blood supply. Patients with high-grade bowel obstructions require an emergency operation to relieve the obstruction before the adverse sequelae of bowel ischemia.
Given the prevalence and morbidity associated with adhesions extensive research have focused on identifying methods to avoid adhesion formation. Adhesions result from trauma to tissues, tissue ischemia, infection within the abdominal cavity, inflammatory processes, or by the presence of foreign bodies such as suture, talc from gloves, and lint from sponges. To minimize adhesions, gentle tissue handling with strict hemostasis and minimization of intraperitoneal trauma are core principles. In addition, frequent irrigation to dilute or to remove contaminants and the use of small, nonreactive suture material will diminish the contribution to adhesiogenesis. Perhaps the most effective method of preventing serious adhesions is via the use of the omentum. The omentum may be used to wrap anastomoses or to protect abdominal contents from a healing midline incision. Despite the adverse effects of adhesion formation, adhesions are an important part of the wound healing and without adhesions most anastomoses would likely fail.
Fistulae
A fistula is an abnormal communication between two epithelized surfaces. A variety of fistulas can exist within the abdomen, including pancreatic and biliary fistulae, fistulae between two intra-abdominal organs, and enterocutaneous and enteroatmospheric fistulae. The majority of GI fistulae occur as complications of abdominal surgery. The incidence of spontaneous fistula formation is rare and is usually the result of intra-abdominal infection or inflammation. The natural history of a fistula begins as a bowel leak. The type of fistula depends on whether the leak is uncontrolled, partially controlled, or well controlled (31). An uncontrolled leak will result in peritonitis and require surgical exploration for correction of the underlying pathology. A partially controlled leak may result in an intra-abdominal abscess, which will require definitive therapy such as open or percutaneous drainage. Controlled leaks result in fistulae. Management of fistulae can be a long-term challenge for surgeon and patient.
An enterocutaneous fistula is an abnormal communication between the bowel and the skin surface. The majority of these fistulae (71% to 90%) are the result of postoperative iatrogenic complications (29,32). Spontaneous causes of fistulae are uncommon but may include malignancy, inflammatory processes, mechanical obstruction, or vascular insufficiency. Iatrogenic fistulae may result from inadvertent enterotomies, intra-abdominal infections, direct injury or bowel desiccation in the open abdomen, misplaced stitches, or anastomotic breakdown. Impaired tissue perfusion from hypotension or vascular disease may predispose to this complication, as will infections, steroids, and malnutrition. Characterization of the fistula tract and surrounding anatomy is essential, best done with a fistulogram. This is done by injecting gastrografin into the tract and using fluoroscopy to follow the progress of the contrast. A fistulogram is useful to define the length of the tract, tortuosity, tract diameter, and which segment of the gastrointestinal tract is involved. A CT scan is helpful in defining surrounding anatomy such as intra-abdominal abscesses, malignancy, and hernias (33).
A postoperative enterocutaneous fistula typically presents as discolored, watery drainage or frank succus from the midline incision. Palpation along the facial closure suture line will often reveal a local dehiscence. Passage of gas from the midline wound is diagnostic of an enterocutaneous fistula. Patients will usually demonstrate signs of infection characterized by increasing temperature, white blood cell count, and persistent ileus. Some patients may develop profound shock due to electrolyte imbalances and sepsis. In these cases, emergent re-exploration is necessary. However, if the patient presents with drainage or an obvious fistula but is hemodynamically stable, a short-period conservative management is reasonable.
Conservative Management of the Enterocutaneous Fistula. Initial management of enterocutaneous fistulas is based on evaluation and control of sepsis, aggressive fluid resuscitation with correction of electrolytes and nutritional deficiencies, and control and characterization of fistula output with protection of surrounding skin surface. Early and aggressive management of these factors will maximize the potential for spontaneous closure. Patients with enterocutaneous fistulae are prone to malnutrition from protein losses, increased metabolic demands, and limited oral intake; early fluid and electrolyte replacement is needed. Parenteral nutrition is often necessary to provide early nutritional repletion, enable management of electrolyte and protein balances, and to decrease volume transit past the fistula in the gastrointestinal tract. Other methods of reducing volume of enteric content past the fistula is the use of narcotics, loperamide, and somatostatin analogs. The use of octreotide or other somatostatin analogs (100 μg intravenously every 8 hours) may decrease gastrointestinal secretions. Somatostatin inhibits the secretion of most gastrointestinal hormones and enhances fluid and electrolyte absorption, thereby decreasing intraluminal volume and potentially decreasing fistula output. Despite the theoretical benefits of somatostatin use, clinical studies have revealed mixed results on effectiveness. Although some studies have demonstrated a decreased fistula output and higher rate of spontaneous closure, an equivalent literature reveals no statistical difference in output or closure rates (34). As side effects are relatively mild, including gastrointestinal discomfort and increased biliary sludge, we recommend trying a somatostatin analog in conjunction with other conservative therapies while waiting for a fistula to close spontaneously.
Containment and control of fistula output is a significant challenge. Enteric contents are extremely caustic to the skin and surrounding tissues, creating a need to isolate enteric contents from the skin. For a simple enterocutaneous fistula, a stoma appliance is usually sufficient. However, many fistulae present in open wound beds, including on granulating abdomens. These tissue fields are not amenable to the placement of a simple stoma appliance. In these situations, a multidisciplinary approach with the surgeon and wound care nurse/enterostomal therapist is needed to control fistula output. Once initial control is achieved, it may be possible to close fistulae surgically or to skin graft the region.
Spontaneous Fistula Closure. Spontaneous fistula closure is the goal of conservative management. Many fistulae close without operative intervention, and will do so in the first 3 to 6 weeks after appearance. The spontaneous closure of a fistula is dependent on its inherent characteristics. Fistulae with long tracts and narrow mouths are more likely to resolve without intervention. Low-output fistulae (less than 500 mL per day) have a higher likelihood of closure than do high-output ones. A fistula with persistent drainage after 3 months is unlikely to close without surgical therapy. In addition, several patient factors are associated with failure of the fistula closure. These include the presence of a foreign body in the fistula tract, close association with an abscess, presence of malignancy, distal bowel obstruction leading to increased pressure and transit through the fistulous tract, and a short neck with wide fistula mouth. Longstanding fistulae with high outputs are unlikely to close spontaneously. To improve the likelihood of spontaneous fistula closure, optimal nutrition for wound healing and minimization of enteric content should be undertaken. Parenteral nutrition is used to decrease the volume transiting the gastrointestinal tract and through the fistula. A positive nitrogen balance and a transferrin level greater than 200 mg/dL are also associated with successful closure (35).
Surgical Therapy for Enterocutaneous Fistulae. Failure of spontaneous fistula closure is considered after 3 months if the fistula remains open; after this point the likelihood of closure without surgical management is poor. Preoperative management requires characterization of the fistula track and surrounding anatomy, optimization of nutrition, albumin and pre-albumin levels, and wound care. Control of fistula output and maintenance of healthy skin integrity at the time of operation will improve the success of abdominal wall reconstruction (34). With careful planning and delay of operative repair until all criteria are met (nutrition, fistula definition, wound care), the morbidity and mortality may be decreased from 50% mortality and 50% recurrence in early surgeries to 94% successful closure and a 4% mortality rate (29,36).
Surgical management of an enterocutaneous fistula requires a laparotomy. Management of intra-abdominal adhesions from prior surgeries or infection is a challenge. Extensive and dense adhesions may make access to the fistula difficult with the risk of enterotomies. While a common initial impulse is to oversew the fistula primarily, this should be avoided whenever possible as the recurrence rate is high. The preferred method for surgical management remains complete lysis of intra-abdominal adhesions and resection of the involved segment. With this approach, the diseased portion of bowel is removed and the anastomosis is performed between two healthy segments of bowel. The complete lysis of adhesions allows careful inspection of the remaining bowel to rule out downstream obstruction or other pathology. Although time consuming, this approach provides the highest likelihood of recovery without recurrent fistulization.
Enteroatmospheric fistulae communicate with an open granulating abdomen and represent a complex management problem. In particular, managing the fistula drainage on a granulating surface makes it difficult to control contamination. Often a multidisciplinary approach with an enterostomal therapist is necessary to identify a functional solution using a variety of stoma appliance options. A split-thickness skin graft is a favorable option for patients with a fistula in the face of the granulating, open abdomen. The skin graft will decrease the metabolic demands of a granulating abdomen and provides a good base for control of fistula output. At the time of skin grafting, the fistula track should be cannulated with a catheter to allow for preferential drainage of enteric content and to avoid contamination of the skin graft site. Contamination of the graft site often complicated with high rate of graft failure. A vacuum assisted closure (VAC) appliance should be applied to the skin graft site with a specialized porous VAC sponge surrounding the fistula opening to prevent injury to the bowel surface; this should be changed every 2 to 3 days.
The Pancreatic Fistula
The majority of pancreatic fistulae result from trauma or pancreatic resection, with only a small percentage resulting from primary pancreatic diseases. The principles of management are diagnosis of the fistula and wide drainage. Evaluation with a CT scan will provide important information about the pancreatic anatomy, degree of inflammation, and peripancreatic fluid collections. Pancreatic fluid contains a large amount of bicarbonate (70 to 90 mEq/L), and inadequate replacement of bicarbonate may lead to nonanion gap metabolic acidosis. Pancreatic fistulae typically drain between 100 and 1,000 mL of fluid/d. Classification of pancreatic fistulae is outlined in Table 58.2 (37). Pancreatic injury may result in accumulation of pancreatic ascites, resulting in abdominal pain, fever, ileus, and abscess formation. There exists a spectrum of patient clinical presentation from a pancreatic leak: some patients may present in profound shock while others may tolerate large-output pancreatic fistulae with a benign clinical presentation. The source of this variability in clinical presentation is poorly understood but is likely due to the degree of enzymatic activation of the leaking fluid.
For most patients, the initial treatment for a pancreatic fistula is percutaneous drainage. Intraoperative concern for a postoperative pancreatic leak should prompt the surgeon to prove wide drainage with a closed-system drain before closing the patient’s abdomen. Wide drainage of pancreatic secretions should allow time for the patient to stabilize and prevent damage to other abdominal organs. Long-term drainage is often needed to enable spontaneous closure of the pancreatic fistula. This conservative approach with drains is generally pursued for up to 6 months and has a success rate of up to 97% in some studies (38). Pancreatic fistulae with persistent drainage should undergo imaging studies to define duct anatomy and determine if an obstructive process is maintaining fistula patency. Magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) may provide similar information; however, ERCP is generally preferred as it enables characterization of duct anatomy and allows for intervention. Stenting of a proximal obstruction may be adequate to allow prograde drainage of pancreatic secretions and closure of the fistula, thereby avoiding surgical therapy (39). Failure of conservative therapy requires exploratory laparotomy for definitive management of a pancreatic fistula. Surgical management depends on the level of the injury. A fistula resulting from the distal duct is treated by distal pancreatectomy. If the leaking duct is sufficiently large, a pancreaticojejunostomy may be performed to allow for a low-resistance drainage pathway. Pancreatic fistulae involving the proximal duct are most often iatrogenic or related to trauma and are troublesome to deal with, in light of other major structures in the region. For these patients, a pancreaticoduodenectomy will resect the leaking portion of pancreas and allow reconstruction. This procedure should only be performed in patients with good physiologic reserve and nutrition. As noted, an attempt at conservative therapy and complete preoperative imaging and optimization are mandatory as these procedures are a major commitment for surgeon and patient (38).
| TABLE 58.2 Criteria for Grading Pancreatic Fistula: ISGPF Classification Scheme |
 |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


