EMERGENCY CHILDBIRTH
When a woman is ready to give birth, the contractions of labor are usually intense and uninterrupted, or separated by intervals of less than 3 to 5 minutes. If the child to be born is not the woman’s first, labor can progress very quickly, so don’t wait until the last minute to set up. On the other hand, don’t deliver a baby in the woods if it isn’t necessary. If the child is the mother’s first, if the contractions are more than 5 minutes apart, if the waters have not “broken” (a gush of fluid from the ruptured amniotic sac) and there has been no passage of bloody mucus, and if no bulging is present in the vaginal area, consider whether you have time to make it to the hospital. If the waters have broken and labor has not begun, it is best to evacuate the mother, because delivery must occur or be induced within 24 hours to avoid the onset of an infection that could jeopardize the infant and mother. If the umbilical cord or any other part of the infant other than the head is showing at the vagina, the delivery will be difficult and should be performed if at all possible by a skilled obstetrician.
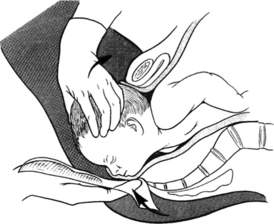
A baby is delivered in (ideally) two stages. First, the head and face appear, usually with the face down (Figure 104). Once the infant has appeared to the level of his eyebrows, instruct the mother to stop pushing. The baby will be extremely slippery. When his face appears, run your fingers around the infant’s neck to see if the umbilical cord is wrapped around it. If it is, see if you can slip it over the head. If not, tie (clamp) it off tightly twice, with about 1 ½ in (3.8 cm) between ties, and cut carefully between the ties. The ties must be tight and not slip off, or the baby could suffer severe bleeding.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


