Chapter 29 Dysrhythmias and Tachyarrhythmias
5 What should you think of when you see a very wide QRS (and no P waves)?
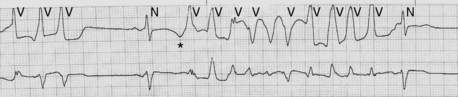
Hyperkalemia leads to baseline depolarization of cardiac cell membranes. This in turn results in an increased proportion of inactivated sodium channels. The global consequence of increased inactivation is decreased conduction velocity. In the atria this creates long low-amplitude P waves (which can be difficult to see), and in the ventricle it creates a very wide QRS. With sufficient hyperkalemia a sine wave–appearing rhythm can result. If the underlying rhythm is fast (e.g., sinus tachycardia) the wide QRS and apparent lack of P waves can be mistaken for VT. It is critical not to give sodium channel blocking antiarrhythmics (e.g., lidocaine) in this setting because they further increase sodium channel inactivation and can result in asystole and death. Treatment should be aimed at stabilizing the cell membrane (calcium) and reducing potassium (insulin, glucose, Kayexalate, and/or dialysis). See Figure 29-1.

6 What is torsades de pointes, and what predisposes a patient to it?
 Constellation of one long QT interval (QTc > 440 ms in men and > 460 ms in women)
Constellation of one long QT interval (QTc > 440 ms in men and > 460 ms in women)
 Initiation with a long-short interval (tachycardia begins after a pause [long cycle])
Initiation with a long-short interval (tachycardia begins after a pause [long cycle])
 Premature ventricular contraction that begins during the T wave (short cycle)
Premature ventricular contraction that begins during the T wave (short cycle)
Long QT (and torsade) can result from a congenital ion channel abnormality or ion channel blocking medication (see Fig. 29-2) and can be exacerbated by hypomagnesemia, hypokalemia, and hypocalcemia.
7 What drugs commonly used in the ICU can cause QT prolongation?
See Box 29-1. See also www.torsades.org.
Box 29-1 Drugs Commonly Used in the ICU that Can Cause QT Prolongation
| Amiodarone | Quinidine |
| Clarithromycin | Sotalol |
| Amitriptyline | Moxifloxacin |
| Haloperidol | Lithium |
| Methadone | Risperidone |
< div class='tao-gold-member'>
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


