Drowning and Submersion Injuries
Adam Cheng MD, FRCPC (Ped EM), FAAP
DEFINITIONS
Drowning: respiratory impairment from submersion or immersion in a liquid.1
Survival is not considered in the definition. The victim may survive or die.
EPIDEMIOLOGY
500,000 drowning deaths occur worldwide annually.2
Annual incidence of drowning in the United States is 15,000 to 70,000.
> 50% of drowning victims are children under 5 years of age.3
Fatality rates are highest in children under 5 years of age.
Males more commonly affected than females.
Leading cause of cardiac arrest in children.
Leading cause of accidental death in children from industrialized countries.
Site of drowning, as reviewed by Brenner and associates in 2001:4
< 1 year: 55% in bathtubs.
1 to 4 years: 56% in artificial pools.
Older children: 63% in natural collections of freshwater.
PATHOPHYSIOLOGY (FIG. 17-1)
Exact pathophysiologic mechanism of drowning remains unclear.
Final common pathophysiologic consequence is hypoxemia.
Hypoxemia results from three main causes:5
Apnea and breath holding.
Laryngospasm.
Pulmonary aspiration and lung injury.
Surfactant disruption.
Alveolar collapse and atelectasis.
Pulmonary edema.
Intrapulmonary shunting.
Ventilation—perfusion mismatch.
Cardiac arrest can ultimately occur from:
Prolonged hypoxia.
Intense peripheral vasoconstriction.
Hypothermia.
Extravascular fluid shifts, and intravascular fluid loss.
Bradycardia.
Ventricular fibrillation or other arrhythmias.
Water tonicity (freshwater vs. seawater) does not influence change in serum sodium, hemoglobin, or intravascular volume status.6
Hypothermia often occurs in drowning, particularly with prolonged submersion.
Below 32°C, heart rate and blood pressure fall and oxygen consumption and metabolic rate decrease.
Severe hypothermia creates risk of bradycardia, ventricular fibrillation, or asystole.
Can lead to coagulopathy and platelet dysfunction.
Protective effect on brain function possible if hypothermia occurs quickly.
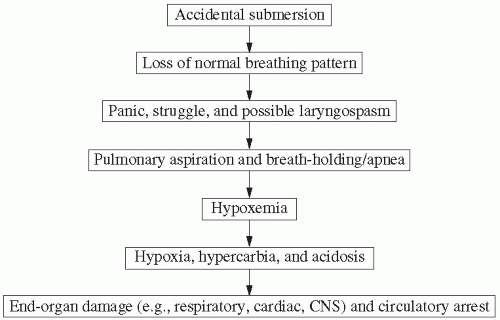 FIGURE 17-1 • Pathophysiologic mechanism of drowning. |
RISK FACTORS FOR DROWNING
Young age, particularly less than 5 years.
Child maltreatment and neglect.
Alcohol intoxication: 40% to 50% of drowning is associated with alcohol use.
Drug abuse.
Seizure disorder: 4 to 5-fold increased risk for submersion.
Cardiac disorder: Prior history of arrhythmias (e.g., long QT syndrome).
Risk-taking behavior.
Residential swimming pool: Location of most drownings in 1 to 4 year age group.
Proximity to rivers, lakes, canals, beaches: Mostly for adolescent age group.
INITIAL MANAGEMENT: PRE-HOSPITAL CARE
At the Scene
Remove from water immediately.
Initiate CPR immediately (bystander resuscitation is critical).
Heimlich maneuver NOT indicated.
Obtain details: Submersion time, symptoms, vomiting.
During Transport
Initiate PALS protocols and cardiorespiratory monitoring.
Airway management.
Protect C-spine: Jaw thrust if needed.
Administer 100% oxygen.
Give IV fluids: Normal saline or Ringer’s lactate.
Remove wet clothing.
Initiate rewarming: Wrap in blankets.
Airway and Breathing
Rapid-sequence intubation (RSI) if indicated:
Apnea, severe respiratory distress, poor oxygenation, PaCO2 retention, altered mental status, inability to protect airway.
See Chapter 3 on Airway Management for RSI technique and medications.
Consider C-spine stabilization for suspicious cases.8Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








