Chapter 13 Complications of Epidural Injections
 Epidural injections for the treatment of chronic pain should only be performed by well-trained physicians under fluoroscopic guidance.
Epidural injections for the treatment of chronic pain should only be performed by well-trained physicians under fluoroscopic guidance.



Introduction
Epidural steroid injections (ESIs) have been associated with a myriad of complications and side effects. Although the overall incidence of complications from ESIs appears to be low,1 there are some potentially catastrophic complications that should be considered by all physicians performing these procedures. There are two general categories of complications associated with ESIs: exogenous steroid side effects and complications associated with the actual placement of the needle by the physician performing the procedure. Complications associated with ESIs are discussed in this chapter and are organized into medication-associated complications and those complications that may result from the procedure.
Complications of Steroid Administration
Complications that may result from corticosteroid injections include hyperglycemia, Cushing syndrome, hypertension, deep venous thrombosis (DVT), secondary infections, psychological disorders, lipid accumulation (epidural lipomatosis), osteoporosis, vertebral compression fractures, avascular necrosis of joints, and numerous other endocrine and dermatologic manifestations.2 Epidural steroid administration has been demonstrated to adversely affect native cortisol concentrations for up to 30 days from a single injection.3 It is likely that suppression of the hypothalamic–pituitary–adrenal (HPA) axis is variable among individuals, but there is evidence that a series of three epidural injections with 40 mg of triamcinolone may suppress the HPA axis for up to 3 months.2 Serious side effects such as steroid myopathy and Cushing syndrome have been reported after a single epidural dose of triamcinolone.4 Although the risk of complications from ESIs theoretically should increase with increasing frequency of injections, it appears that total dose of steroids given during a specific time may be more important in determining steroid complications.5,6
Recommendations for Avoiding Steroid Complications
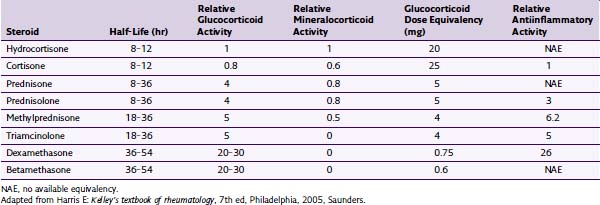
The total annual dose of steroid should be limited to the smallest efficacious dose. Although there is insufficient evidence to determine the risks of epidural steroid administration, evidence suggests that large annual doses of steroids may lead to serious complications. There is no evidence that large doses of steroids are superior to low doses. Recommendations have been made to limit the amount of annual steroid dose to 3 mg/kg of triamcinolone or equivalent.7 See Tables 13-1 and 13-2 for commercially available steroid preparations and their relative potencies.
Table 13-1 Commercially Available Steroids
| Steroid | Available Concentrations (mg/mL) | Typical Doses (mg) |
|---|---|---|
| Depo-Medrol (methylprednisolone) | 40, 80 | 40–80 |
| Celestone (betamethasone) | 6 | 6–12 |
| Kenalog (triamcinolone) | 25, 40 | 40–80 |
| Decadron (dexamethasone) | 4, 8 | 4–10 |
Adapted from Deer T, Ranson M, Kappural L, Diwan SA: Guidelines for the proper use of epidural steroid injections for the chronic pain patient, Tech Reg Anesth Pain Manage 13(4):288-295, 2009.
Transforaminal ESIs, especially in the cervical spine, have been reported to result in catastrophic complications, including stroke, paralysis, and death.8 Although there are more case reports of complications with transforaminal injections in the cervical spine, there are some reports of neurologic injury in the lumbar spine.9 Several mechanisms have been proposed for the development of anterior spinal artery syndrome, including mechanical trauma to a radicular artery supplying the anterior or posterior spinal arteries, vasospasm, and embolism resulting from particulate-containing steroids (Figs. 13-1 and 13-2).10,11 The use of nonparticulate steroids has been suggested to be safer than particulate steroids when performing cervical transforaminal injections.12 Cervical transforaminal injections should be approached with caution,7 and prudent physicians should consider using nonparticulate steroid solutions such as dexamethasone when performing transforaminal epidural injections in the thoracic and upper lumbar spine.
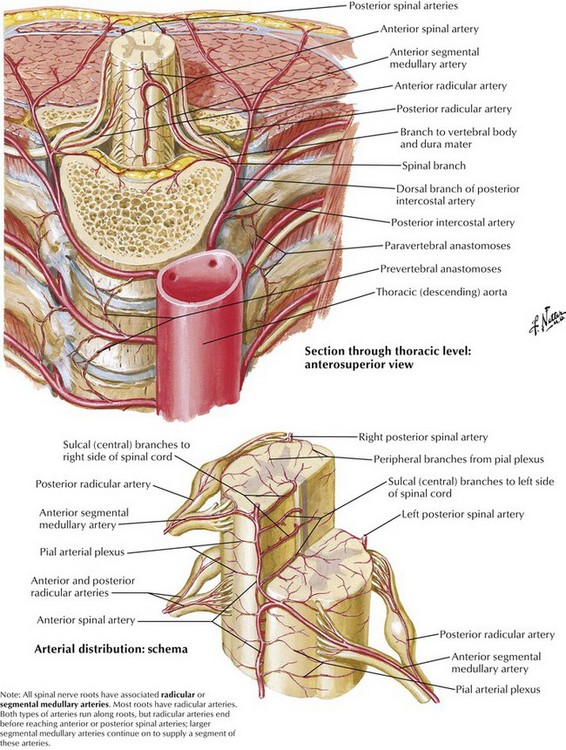
Fig. 13-1 Arteries of the spinal canal and epidural anatomy.
(Netter illustration from www.netterimages.com. © Elsevier, Inc. All rights reserved.)
Related posts:
 Radiation Safety and Complications of Fluoroscopy, Ultrasonography, and Computed Tomography
Radiation Safety and Complications of Fluoroscopy, Ultrasonography, and Computed Tomography
 Complications of Sacroiliac Joint Injection and Lateral Branch Blocks, Including Water-Cooled Rhizotomy
Complications of Sacroiliac Joint Injection and Lateral Branch Blocks, Including Water-Cooled Rhizotomy
 Complications Associated with Head and Neck Blocks, Upper Extremity Blocks, Lower Extremity Blocks, and Differential Diagnostic Blocks
Complications Associated with Head and Neck Blocks, Upper Extremity Blocks, Lower Extremity Blocks, and Differential Diagnostic Blocks
 Complications of Lumbar Spine Fusion Surgery
Complications of Lumbar Spine Fusion Surgery
 Complications Related to Radiofrequency Procedures for the Treatment of Chronic Pain
Complications Related to Radiofrequency Procedures for the Treatment of Chronic Pain
 Complications of Therapeutic Minimally Invasive Intradiscal Procedures
Complications of Therapeutic Minimally Invasive Intradiscal Procedures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


