A. Most complications of myocardial infarction (MI) and the highest associated mortality occur in the first few months after the acute event; therefore, prompt identification and treatment of any established or potential complications are necessary. An overview of the most common complications is presented in Table 34-1.
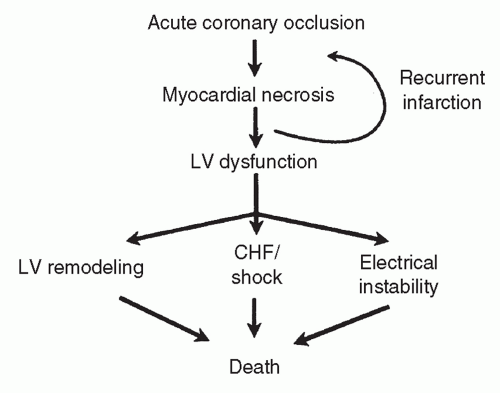
II. PATHOPHYSIOLOGY: The proximate cause of ST elevation MI (STEMI) in most patients is acute coronary occlusion resulting from plaque rupture and platelet-initiated thrombosis. A non-ST elevation MI (NSTEMI) occurs when a nonocclusive thrombus develops. The sequelae of coronary occlusion are depicted in Figure 34-1.
III. PROGNOSIS AFTER MI
A. Incidence of complications has decreased in the reperfusion era. Recent registries indicate that the 30-day mortality following an STEMI is as low as 4.4%, whereas the mortality following an NSTEMI is 5%.
B. The thrombolysis in myocardial infarction (TIMI) study group recognized predictors of mortality after STEMI: age, low body weight, tachycardia, hypotension, history of hypertension, diabetes, or angina, time to treatment, anterior MI, MI with new left bundle branch block, and development of heart failure (HF). Similarly, they recognized the following predictors of mortality after NSTEMI: age, ≥3 CAD risk factors, known CAD with >50% stenosis, aspirin use in the last 7 days, severe angina in the last 24 hours, elevated cardiac markers, and ST deviation >0.5 mm.
C. An alternative index of mortality after either a STEMI or NSTEMI is the GRACE risk model that includes the following predictors: age, Killip class, systolic BP, presence of ST-segment deviation on admission, cardiac arrest at presentation, serum creatinine, elevated cardiac biomarkers, and heart rate.
IV. RECURRENT ISCHEMIA OR INFARCTION
A. Incidence and clinical consequences: Recurrent ischemic events after acute MI are a major cause of subsequent mortality. Reinfarction occurs in 4% to 10% of patients after thrombolytic therapy and 2% to 5% of patients after percutaneous coronary intervention (PCI) with most cases occurring within 4 days of hospital admission.
TABLE 34-1 Complications Following Acute MI
Recurrent infarction or ischemia
Infarct expansion
Thinning and dilation of infarct segment without pain or CK leak
Infarct extension
Recurrent pain, ECG changes, and CK-MB leak
Left ventricular dysfunction
Acute
Diastolic dysfunction may lead to pulmonary edema
Systolic dysfunction may lead to cardiogenic shock and be a nidus for LV thrombus formation
Chronic
LV dilation and remodeling
LV aneurysm and pseudoaneurysm
LV thrombus
Inferior MI complications
RV infarct physiology
Preload-dependent hypotension, increased JVP, and clear lungs; Kussmaul sign often present
Heart block
High-degree AV block
Mechanical complications
Free wall rupture
VSD
Papillary muscle rupture causing acute MR
Electrical disturbances and conduction disorders
Ventricular tachycardia and ventricular fibrillation
Atrial fibrillation (10%-17% incidence)
Conduction disorders and bradyarrhythmias
Miscellaneous
Complications of angiography and PCI such as access site bleeding, renal failure, vascular or coronary dissection, and cholesterol emboli syndrome
Thromboembolism
Pericarditis/Dressler syndrome
LV, left ventricle; CK, creatinine kinase; MB, MB fraction of creatinine kinase; ECG, electrocardiogram; RV, right ventricle; JVP, jugular venous pressure; AV block, atrioventricular block; VSD, ventricular septal defect; MR, mitral regurgitation; PCI, percutaneous coronary intervention.
B. The consequences of reinfarction with regard to short- and long-term mortality are grave. In the Multicenter Investigation of Limitation of Infarct Size (MILIS) study, patients who had infarct extension had an in-hospital mortality more than fourfold higher than patients without extension (30% vs. 7%, p < 0.01).
Figure 34-1. Sequelae of coronary artery occlusion. LV, left ventricle; CHF, congestive heart failure.
C. Prevention.
1. Antithrombotic therapy.
a. Platelet inhibition is one of the cornerstones of antithrombotic therapy in MI patients. Aspirin been shown to be of benefit across a wide spectrum of patients with ischemic heart disease. The antiplatelet agents clopidogrel, prasugrel, and ticagrelor provide further benefit when added to aspirin in patients with acute coronary syndrome (ACS), particularly those undergoing PCI.
b. Glycoprotein (GP) IIb/IIIa inhibitors are additional inhibitors of platelet aggregation and may be used in conjunction with PCI; in contrast, GP IIb/IIIa agents do not provide benefit when used with thrombolysis.
c. The next component of antithrombotic therapy for prevention of recurrent infarction is anticoagulation. Intravenous unfractionated heparin is necessary to maintain infarct-related artery patency in patients undergoing thrombolysis or PCI. Alternatives to UFH include low molecular weight heparin (LMWH), direct thrombin inhibitors (DTI) such as bivalirudin, and the pentasaccharide fondaparinux. Bivalirudin in particular has been shown to have similar ischemic outcomes and reduced bleeding as compared with UFH in patients with MI undergoing PCI.
2. β-Blockade has been studied extensively and has been found to be beneficial, especially among patients at highest risk, such as those with a history of HF or ventricular arrhythmias after MI. Oral β-blockade should be provided to all patients without contraindications (e.g., bradycardia, cardiogenic shock, severe HF, hypotension, second-/third-degree AV block). IV β-blockade may be given to those with tachyarrhythmias or uncontrolled severe hypertension (in the absence of contraindications), although care must be given as beta-blocker treatment in the acute setting may increase the risk of HF or shock.
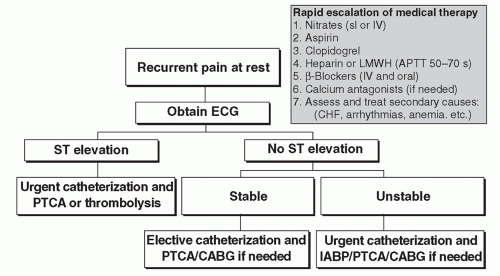
D. Treatment: An approach to the acute evaluation and treatment of recurrent ischemic events is outlined in Figure 34-2.
Figure 34-2. An approach to the acute evaluation and treatment of recurrent ischemic events. Sl, sublingual; IV, intravenous; LMWH, low molecular weight heparin; APTT, automated partial thromboplastin time; CHF, congestive heart failure; ECG, electrocardiogram; PTCA, percutaneous transluminal coronary angioplasty; CABG, coronary artery bypass graft; IABP, intraaortic balloon pump.
V. RIGHT VENTRICULAR INFARCTION
A. Background: Right ventricular (RV) infarction occurs clinically in approximately 30% of patients with inferior MI (themselves accounting for more than half of all MIs), but only in half of those cases is it clinically relevant.
B. Pathophysiology.
1. RV infarction is caused by very proximal occlusion of the right coronary artery.
2. A loss of contractile performance of the RV—a thin-walled chamber— results in reduced left ventricular (LV) preload and systemic hypotension. The associated diastolic abnormalities cause systemic venous hypertension.
3. Atrioventricular (AV) or sinoatrial (SA) nodal block occurs in 10% to 15% of patients with inferior MI but is particularly prevalent in those with RV infarction; approximately 25% of patients with inferior MI with RV involvement develop conduction system disease.
C. Clinical presentation.
1. Jugular venous distension (JVD) and clear lungs distinguish RV infarction from combined right- and left-sided congestion resulting from LV dysfunction.
2. Systemic hypotension is a frequent complication of RV infarction, in which poor RV output leads to decreased LV filling.
3. Right-sided electrocardiogram (ECG) may facilitate diagnosis. ST elevations in lead V4R in particular should raise suspicion. Precordial ST-segment depressions can be seen on the ECG of patients with RV infarction in 15% to 30% of cases and must be differentiated from anterior ischemia.
4. The differential diagnosis for RV infarction includes hypotension resulting from LV infarction, pericardial tamponade, constrictive pericarditis, and pulmonary embolism (PE).
D. Treatment.
Only gold members can continue reading. Log In or Register to continue