“Collateral damage” goes beyond injury and death. The fragile and superficially placed piping seen in the foreground was the main water artery to this village in Iraq. Public health infrastructure may be different than the normal standard for civilian contractors, the military, and aid workers. Public health “indirect” deaths are more prevalent than direct deaths from weaponry and violence.
In contrast to direct indices, indirect deaths are rarely measured, are more functional and abstract in nature, frequently require qualitative or semi-quantitative measures, and their accuracy is difficult to confirm. In CHEs, the health system and public health infrastructure is the first to be destroyed and last to recover or be rehabilitated. In the post-conflict phase, the risk of continuing death and disability from environmental, communicable, and noncommunicable diseases related to the lack of this recovery may continue to decay up to 10 years post-conflict and the effects may far exceed the immediate loses from the war itself.8,9 Similar consequences are found in countries contiguous to the conflict.
Despite the cessation of hostilities, subtle and rarely counted mortality and morbidity result from those now out of work and despondent, demobilized soldiers, and IDPs who are more likely to suffer suicide, depression, and alcohol and drug use. A sensitive marker of the continued community decay and economic and physical insecurity is an increase in sex-based violence among intimate partners.10 In developing countries experiencing residual post-conflict insecurity, families struggling to recover economically will frequently delay reenrollment of their children to school, usually females – a factor that subtly correlates with high child mortality rates. Over the past decade, humanitarian assistance has moved from insecure rural Africa and Asia to overcrowded urban areas.11
Urban aid is predominantly focused on protecting single or widowed mothers with young children seeking some semblance of security, education, and essential public health and social services after their rural economies are destroyed. Many have been forced to resort to prostitution to avoid abject poverty, and then commonly contract sexually transmitted diseases. The increased density of urban populations has rapidly outstripped the fragile and poorly maintained public health infrastructure. Few urban conclaves have safe water and sanitation. More than 2.5 billion people, almost one of every two people in the developing world, do not have adequate water and sanitation.11 Globally, nearly 4,000 children die each day from unsafe water and lack of basic sanitation facilities.11 In areas where the vector exists, outbreaks of dengue fever serve as a marker of economic decay and worsening governmental services resulting from increased breeding of mosquitoes in the stagnant water of failed public rubbish collection systems.12
Achievement Indicators
Achievement indicators refer to the completion of certain humanitarian-related missions, such as emergency delivery of military rations and rebuilding of clinics and hospitals. Coalition military and private contractors prefer to use achievement indicators rather than outcome indicators in measuring effectiveness of their interventions. Achievement indicators do not necessarily result in improved outcomes or guarantee the functional return of the health and public health infrastructure. Whereas these functions are critical to the relief process, claims of success in humanitarian aid and reconstruction must be viewed with caution when achievement indicators alone are used.
Epidemiology of CHEs
CHEs can be divided into developing, smoldering or chronic country, and developed models, all with differing data presentations.2,4 Models are valuable in predicting priorities for immediate aid, even before confirming field level assessments. There are overlaps in these three models, especially when developed country conflicts persist with failed public health infrastructure, resulting in failing indices similar to those seen in developing countries. Iraq once enjoyed stable health indices indicative of a developed country. In 2007, after 4 years of war and a worsening public health infrastructure, the infant mortality rate equaled that of Afghanistan and Sierra Leone.13 Reported acts of genocide, ethnic cleansing, and torture are a common element of all models of CHEs.
Developing Country Model
Developing country CHEs primarily occur in central Asia and Africa and are characterized by a health profile that exacerbates preventable diseases, such as infectious diseases and malnutrition, resulting from lack of protective levels of food, water, sanitation, shelter, and healthcare (Table 27.1).14 This results in high crude mortality rates, the majority coming from deaths of children younger than 5. Seventy-five percent of the world’s epidemics occur during CHEs.2 Outbreaks typically occur from unprotected endemic diseases. The major causes of mortality and morbidity are diarrhea and dehydration; malnutrition and micronutrient diseases such as vitamin A, C, and B6 deficiencies; complications from childhood vaccine-preventable diseases such as measles and tetanus; complications from acute respiratory infections; and malaria (Figures 27.2, 27.3–27.5, 27.6–27.7, 27.8, 27.9, 27.10, 27.11, 27.12, 27.13).
Developing Country Health Profile
|

Although considered a common and treatable problem in the western world, impetigo patients are triaged as urgent in refugee camps and among internally displaced populations, especially if the victims are malnourished. Impetigo can progress rapidly from a minor skin infection to septicemia when micronutrient deficiencies and severe malnutrition exist.

Scurvy, or vitamin C deficiency and other micronutrient deficiencies (especially A and B1) must be suspected in prolonged war where malnutrition exists. These cases, seen in Vietnam in the 1960s presented as minor bruising, severe pain when the limbs were moved, and fragile tongue lesions that easily bled. Similar cases were seen in East African camps in the 1990s when the waste diet given to refugees lacked micronutrient supplements. Vitamin C serves as a coenzyme in the metabolic reaction of clotting. Once parenteral vitamin C was administered, the pain from bleeding under the periosteum rapidly ceased.

Severely dehydrated children exhibiting extreme loss of skin turgor. Examples of dehydration and malnutrition are common in complex emergencies, especially in Africa and Asia.

A Kurdish child with severe dehydration from diarrhea. The diagnostic “old man facies” occurs with severe loss of body water and electrolytes. Further examination was not allowed. Confirmatory laboratory tests are rarely available. These cases are usually field-managed as isotonic losses with oral rehydration. With clinical improvement the family trusted the physician to complete the physical examination.

Bubonic and septic plague and other endemic infectious diseases are common when the public health infrastructure is destroyed by war and conflict. This figure illustrates an axillary bubo. Gram stain confirmed Gram negative bipolar rods.

The humanitarian community must be sensitive to cultural beliefs that are not dismissed as modern medical care is added. In this toxic and comatose child, an inguinal bubo was surrounded with a lime substance believed to prevent spread. A paste material was placed over the umbilicus with “Chinese medical writings” as petitions to the “evil spirits” that caused disease. Onion flakes were placed in the hair for fever. The child had a febrile seizure immediately after this photo was taken. The mother, thinking that I had provoked an evil spirit within her child with the foreign instrument (camera) I held in my hand, fled with her child. The mother only agreed to return the child for treatment if I was removed as the healthcare provider. This being impossible, I managed the case from a distance through locally trained assistants.

A case of highly contagious pharyngeal bubonic plague stemming from a cervical bubo with visible flea bite site.

Vaccine preventable diseases are common. Tetanus arising from a foot lesion caused severe lockjaw in this 10-year old male. Hyperventilation with nasal flaring resulted in secondary tetany. This child survived with parenteral penicillin and antitoxin.

Tuberculosis is commonly seen and may result in many secondary cases in crowded camps. This child exhibits both Pott’s disease and a scrofula lesion of the neck.
CHEs result in people attempting to flee the war and conflict. If they flee their homes but are unable or unwilling to cross the country’s border they are termed IDPs. With international law they remain under the authority of the host country, even though national forces may be attempting to find and kill them. This contradiction remains a dilemma for the international community, a well-known illustration being the forced abandonment of fleeing Tutsi civilians by UN peacekeeping forces in Rwanda. Characteristically, IDP mortality and morbidity rates are among the highest. Nongovernmental organizations (NGOs) have difficulties gaining access to IDPs and, in their attempts, often face danger from national or rebel forces. Populations who cross borders to flee death and prosecution are given refugee status under international law and the protective UN agency benefits, both physical and political, that these provisions provide. Once international programs are in place in refugee camps, the health indices begin to improve and in time may prove better than the neighboring country housing the camps. Crucially, similar aid programs must benefit the surrounding countryside to prevent resentment and new hostilities from erupting.
Primary care, public health and preventive medicine, infectious disease, obstetrical, and emergency medicine, all adapted to a resource poor environment, are the skills required of expatriate healthcare assets.15 The World Health Organization (WHO) provides immediate assistance in the form of Emergency Health Kits that provide basic health supplies for a population of 10,000 for 3 months. Additional surgical and safe birthing kits are available.
Smoldering or Chronic Country Model
Countries such as Sudan, Haiti, and Gaza have experienced high levels of conflict for many decades, resulting in a suboptimal health profile (Table 27.2) with characteristics of a country suffering both developmental failure and ongoing requirements for all basic public health services (food, water, sanitation, shelter, health, and fuel) essential for survival. Absent or poorly maintained public health infrastructure results in chronic and untreated survivors of preventable diseases. Expatriate health workers and NGOs frequently serve as the rudimentary public health system for the country, but are often prevented by insecurity from providing care to persecuted and minority groups. Communicable diseases within these countries, other than HIV/AIDS, are similar to those seen in the developed world in the early 1900s.
Smoldering or Chronic Country Model Health Profile
|
Because of chronic high vulnerability, these countries are more prone to adverse consequences of disasters. Haiti has suffered from increased deforestation and lack of tree-root structures that serve to protect other countries from worsening floodwaters. In recent years, uncontained floodwaters resulted in between several hundred to more than 3,000 preventable deaths from mudslides and drowning. A dilemma for the international community has been the frustration of responding to an emergency situation within a country that chronically suffers smoldering environmental decay. The environment suffers incrementally with each added conflict or environmental insult (e.g., drought, famine, post-hurricane flooding). Current disaster terminology may not accurately describe the problems that exist. As with Haiti and Sudan, it is unclear whether to describe these events as emergencies or as more as developmental crises. A category is needed to connote the situation of an inability of the international community, mainly restricted by existing international sovereignty laws, to intervene on the behalf of innocent civilians who may never see a sustainable lifestyle.
This model results in a chronic excess of younger than age 5 death rates. Rebel force violent surges result in an increase in adult direct death rates that often represent ethnic cleansing. A return to the chronic epidemiological picture occurs when the fleeing IDPs and refugees again succumb to preventable deaths and increased morbidity from an environment of barren desert conclaves and hastily built refugee camps (Figures 27.14–27.16).

Refugee Camp Conditions in Northern Iraq, 1992. Camp demographics are critical in determining requirements and vulnerability. As Kurdish men were killed by Saddam’s Iraqi forces, or were fighting to keep their own territory safe, the fleeing Iraqi Kurds were primarily children (50%), women (30%), and the elderly (20%). Logistics and healthcare in the precarious camp tents placed on the side of mountains had to adapt to unique needs.
Required professional expatriate assets are similar to that following an acute emergency in a developing country.15 Without emphasis placed on stable governance and long-term nation-state development, including education and training of indigenous healthcare workers, these countries risk repeating similar emergency crises over and over again.
Developed Country Model
Prior to recent warfare, the former Yugoslavia, Chechnya, and Iraq enjoyed health profiles similar to that of Western industrialized countries (Table 27.3). As with the previous two models, worsening political violence results in IDPs and also refugees seeking permanent asylum in willing countries. The dominance of advanced weapon–related deaths is characteristic of this model. When these weapons are fired in an indiscriminate manner, the resulting deaths by the age and sex epidemiology should reflect their representation within the baseline population demographics; however, epidemiological studies in Kosovo showed excess death rates in patriarchal males and young adult males of military age. This study became pivotal in Hague war crime trials as evidence of targeted ethnic cleansing.16
Developed Country Model Health Profile
|
In the former Yugoslavia, the elderly population resisted displacement and often showed rapid decline in health due to under-nutrition, stress-related mental health conditions, and exacerbation of chronic diseases such as diabetes, hypertension, and cardiac disease as violence separated them from sources of their medications. Ethnic cleansing methods resulted in rape, abductions, and assassinations. Interestingly, epidemics are uncommon in this model, in part because the educated population is aware, even in the worst of conditions, of the need for some semblance of basic hygiene including hand washing.
With worsening security, attacks against civilian and military targets include increasingly lethal improvised explosive device attacks and landmine detonations. Victims exhibit unprecedented multi-organ high-velocity blast effects. Fragile civilian health systems lack the capacity to manage complicated resuscitations for multiple organ failure, multiple limb loss, acute respiratory distress syndrome, and traumatic brain injury and the specialized care required for prolonged recovery and rehabilitation.
With the emphasis on traumatic casualties, the international requirements for aid include emergency medicine, surgical, and anesthesia specialties (Figures 27.17 and 27.18).15 Such services and resources rarely arrive from outside the country before 3 days’ time. The best programs are those that use previously educated and trained indigenous healthcare providers. These local personnel assume augmented responsibilities for emergency healthcare and stabilization during and immediately after the traumatic event, with delayed surgery, intensive care, evacuation, and other interventions provided by the international community. It is essential that international responders provide necessary skill training to local healthcare providers so that the level of competency remains improved even after the international “experts” leave.
Communicable Diseases in CHEs
Connolly and colleagues found that communicable diseases, alone or in combination with malnutrition, account for most deaths in CHEs.17 Disease transmission is promoted by poor and dense population conditions common to refugee camps (Figures 27.14, 27.15, and 27.16). Refugees fleeing the slaughter from small arms and machetes in Rwanda rapidly crowded makeshift camps across nation-state borders. A camp at Goma, in the former Zaire, surged to a population of more than 300,000 in 5 days. Crowding contributed to outbreaks of dysentery and cholera that killed thousands more. Whereas effective interventions are often possible in camp settings, populations covering large and poorly accessed geographical areas or entire countries pose a greater challenge. Health workers, at a minimum, must have an operational understanding of communicable diseases and the management in austere environments of diarrheal disease (watery, bloody, and non-bloody) and dehydration, acute respiratory infections, measles, tetanus, malaria, meningitis, tuberculosis, HIV/AIDS, viral hemorrhagic fevers, cholera and dysentery, and trypanosomiasis and leishmaniasis.
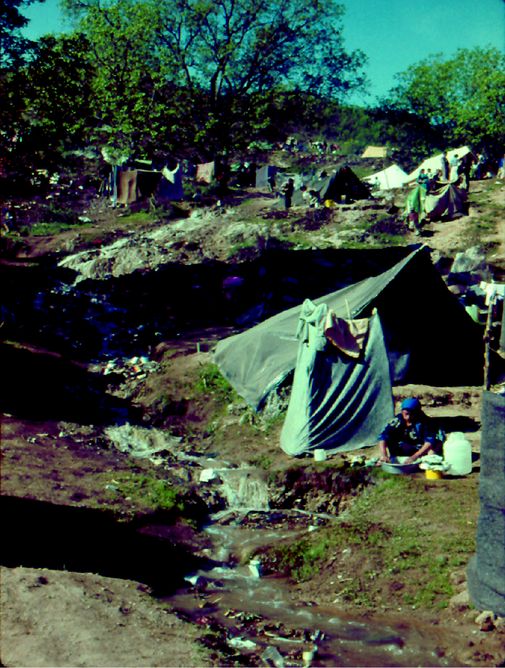
This figure illustrates camp conditions that contributed to 80% of childhood deaths resulting from diarrhea and dehydration secondary to common waterborne bacteria and viruses. Water from melting snow that ran through the camp was polluted by makeshift toilet facility runoff and the washing of soiled laundry.

Mountain streams ended up as stagnant and polluted pools at the base of the camp where children played. Simple and easily corrected public health solutions must be sought to prevent outbreaks.
Standard case definitions for these diseases are critical to reduce variability in reporting. Epidemiological studies confirm, for example, that control of diarrheal diseases occurs through provision of clean water, simple hygiene practices, and sanitation systems; distribution of soap; training of clinical staff and indigenous health workers in aggressive rehydration therapies; and improved basic health services and disease detection. Western medical and nursing personnel generally lack education and training in tropical disease diagnosis and management, and lack experience with the manner in which HIV/AIDS, tuberculosis, and malaria first present with advanced complications in a resource poor environment. Management of region-specific pharmaceutical resistance must be researched before deployment, with special attention to malaria resistance and to the less frequent clinical presentations of tropical diseases such as dengue fever and Japanese B Encephalitis (Southeast Asia), and leprosy (Sudanese refugees).
There are three key elements to humanitarian interventions in communicable disease.17
1. Prevention and control of communicable disease
a. Adequate campsite planning and shelter
b. Water and sanitation
c. Immunization
d. Vector control
e. Epidemic preparedness and response
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


