Key Clinical Questions
How is pneumonia diagnosed?
How should the decision be made to hospitalize the patient?
What are the major infectious causes of community-acquired pneumonia?
What empiric antibiotic therapies are appropriate in community-acquired pneumonia?
What steps should be taken for patients not responding to usual therapy for community-acquired pneumonia?
Introduction
Almost a million episodes of community-acquired pneumonia (CAP) occur each year in the United States in patients over the age of 65 years. While most clinicians are familiar with CAP, its diagnosis remains imprecise, its microbiology is often elusive, and management is usually empiric. Pneumonia is defined as a lung infection, characterized by cough, fever, and a pulmonary infiltrate, often with sputum production. If this sounds obvious, the reader is too easily deceived. Patients with pneumonia may not cough, a variable proportion have sputum, elderly patients are usually afebrile when first evaluated, and infiltrates may be hard to detect, especially in high-risk adults with chronic lung disease, the obese, or those for whom only a portable chest radiograph is available.
To complicate matters, many noninfectious illnesses are also characterized by cough, fever, and pulmonary infiltrates. Some of these are even called pneumonia, such as cryptogenic organizing pneumonia, sarcoid pneumonia, and lupus pneumonitis, and they may in every way mimic pneumonia as already defined. Taken together, all these infectious and noninfectious conditions cause what could be called a pneumonia syndrome. The more experienced recognizes the diverse etiologies of the pneumonia syndrome and should be unhappy about pigeonholing a patient under the rubric of CAP without considering other etiologies.
Pathogenesis
An array of host factors protects the lower respiratory tract against inhaled or aspirated organisms. The predisposition to pneumonia increases to the extent that these factors are altered or bypassed.
The configuration of the upper airways ensures that a thin, laminar flow of air passes close to hairs and sticky surfaces that can trap potentially infectious particles. Secretory immunoglobulin A (IgA), which constitutes 10% of the protein in nasal secretions, neutralizes viruses. These and other immunoglobulins appear to prevent bacterial colonization, probably by blocking binding sites on bacterial surfaces. Closure of the epiglottis prevents food particles from passing into the trachea during swallowing. The larynx prevents the passage of secretions into the trachea and allows the generation of intrapulmonic pressure needed for an effective cough. When particles bypass these mechanisms, ciliary action of epithelial cells moves them steadily upward toward the larynx; the cough reflex propels them more rapidly in the same direction. Tracheobronchial secretions maintain moist surfaces, and pulmonary surfactant probably helps to prevent atelectasis, which might interfere with clearance distally.
When infective agents bypass these mechanisms and reach the alveoli, several innate (nonspecific) and specific defenses come into play. Cells that line the respiratory tract produce substances that kill microorganisms or opsonize them for phagocytosis, including lysozyme, lactoferrin, beta-defensins, and surfactant. Bacterial cell wall components, such as lipopolysaccharide in gram-negative and peptidoglycan in gram-positive bacteria, activate the alternative complement cascade, leading to opsonization and killing of bacteria. They also upregulate toll-like receptors, with subsequent enhancement of humoral and cellular immune mechanisms. Antibodies to bacterial cell wall components greatly enhance the host defense response; serotype-specific antibodies are especially important in host defenses against the pneumococcus.
One way of putting these defense mechanisms into perspective is to consider animal models of infection. Some strains of Streptococcus pneumoniae are lethal if a few viable organisms are injected into the peritoneal cavity, but in order to produce infection by inhalation, an inoculum of 103 or 104 colony-forming units may be required. Other microorganisms resist all defense mechanisms. For example, a single inhaled Mycobacterium tuberculosis organism that lodges in the alveoli establishes infection in guinea pigs and is thought to do the same in humans.
Extremes of age may be the most important risk factor for pneumonia (Table 189-1).
|
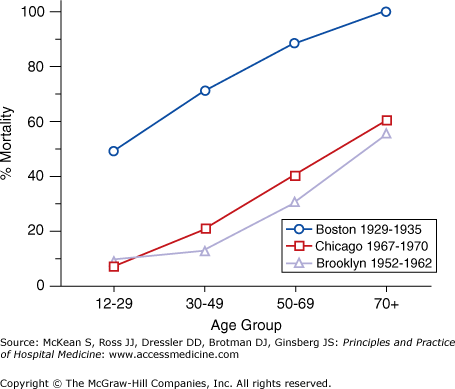
Pneumonia is most common among children under the age of 2 and the elderly. Not only is bacterial pneumonia, exemplified by pneumococcal infection, more common in the elderly, it is also more severe, with the risk of death rising steadily through adulthood (Figure 189-1).
Factors predisposing the elderly to pneumonia include diminished gag and cough reflexes, poor glottal function, diminished toll-like receptor responses, and less robust antibody responses. Pneumococcal pneumonia generally does not affect perfectly healthy young adults. Most adults with pneumonia have one or more predisposing underlying conditions. Even when outbreaks of pneumococcal pneumonia occur among presumably healthy adults, as in military camps, concurrent viral infection, exhaustion, and emotional stress are all thought to play a contributory role. In contrast, viral pneumonia occurs when organisms are transmitted to immunologically naïve hosts, with the presence or absence of humoral antibody as the principal determinant of immunity, rather than age.
In bacterial pneumonia, the host inflammatory response causes most of the disease manifestations. The presence of bacteria and the accumulation of inflammatory cells and cytokines initiate a vicious cycle in which additional inflammatory cells are attracted and further cytokine release is stimulated. These substances cause capillary leakage with exudation of plasma into the alveoli, leading to a progressive inflammatory exudate that is detected radiologically as pneumonia.
Microorganisms other than bacteria cause pneumonia by other means. Influenza virus directly invades columnar epithelium cells, resulting in pathologic changes that range from vacuolization of some respiratory epithelial cells to desquamation of the entire epithelial layer. These changes are diffuse, leading to an interstitial pattern on chest radiograph. They also predispose to secondary bacterial invasion, which is thought to have caused the staggering death rate during the influenza outbreak of 1918–1919. Chlamydophila pneumoniae adheres to specific receptors and replicates within cells, producing microcolonies that stimulate an inflammatory response upon release, with a resulting focal pneumonia. Mycoplasmas also damage respiratory epithelial cells. Rather than invading cells, they adhere to the cell surface, impairing ciliary activity and generating toxic substances. Secondary bacterial pneumonia is uncommon, perhaps because mycoplasmas do not adversely affect phagocytic cells as influenza viruses do. Fungal and mycobacterial pneumonia are dealt with elsewhere in this volume.
Etiology
If pneumonia is defined as an acute or subacute condition characterized by a pulmonary infiltrate accompanied by systemic symptoms, fever, and cough, the list of possible causes is great (Table 189-2).
| Common | Less Common | Uncommon |
|---|---|---|
|
|
|
The prudent physician should give at least brief consideration to other causes before concluding that a “typical” case of CAP merits treatment with “recommended empiric” therapy.
Streptococcus pneumoniae remains the most common cause of pneumonia leading to hospitalization, causing 50–60% of cases, down somewhat from years before widespread use of the conjugate pneumococcal vaccine in infants and toddlers. Literature claiming that pneumococcus causes a far smaller percentage of cases is often derived from case series in which good specimens for bacterial culture were not regularly obtained, but viral cultures (which can be done from nasopharyngeal swabs) and serologic studies were done on most or all patients. Among other bacterial causes, Haemophilus influenzae and Moraxella catarrhalis are the next most common but generally cause pneumonia only in persons who have preexisting lung disease. Staphylococcus aureus pneumonia presents either as a segmental or lobar pneumonia or as a multiple, small cavitating emboli secondary to an intravascular infection. Pseudomonas aeruginosa and other gram-negative rods cause pneumonia in persons with extensive chronic lung disease or treatment with corticosteroids, as well as in immunocompromised hosts, patients with cystic fibrosis, and infrequently in severe alcoholics.
Evidence for viral infection is found in about 15% of adults hospitalized for CAP, of whom about one-half also have bacterial infection. As patients with influenza pneumonia might benefit from antiviral treatment, even if initiated > 48 hours after the onset of symptoms, clinicians should consider diagnostic testing for influenza in the presence of suggestive features, such as prominent muscle aches, headache, a dry cough, and high community influenza activity. Respiratory syncytial virus and human metapneumovirus are the next most common viruses causing hospitalization for pneumonia but are currently untreatable. Although Mycoplasma and Chlamydophila pneumoniae may be common in the ambulatory setting, this author regards them as infrequent causes of pneumonia leading to hospitalization. The current literature, based entirely on serologic studies, overemphasizes their importance. Serologic diagnosis of Chlamydophila infection is proven to be unreliable, and diagnosis has only rarely been based on simultaneous study of paired acute and convalescent serum in the same laboratory.
Epidemiologic clues may suggest specific etiologies of a pneumonia syndrome. Coccidioides immitis, found in arid regions of the Americas, or Histoplasma capsulatum, found worldwide but especially in river basins of North America, cause a variable proportion of CAP in endemic regions. Exposure to livestock or late summer residence in a hot and dry ranching area suggests Coxiella burnetii (Q fever), especially if severe headache and abnormal liver enzymes are associated. Exposure to sick birds raises concern for Chlamydia psittaci. Prolonged cough, low-grade fever, and a pulmonary infiltrate in a parent whose children have similar symptoms suggests Mycoplasma or adenovirus. Mycobacterium avium, a well-known cause of pneumonia in patients with bronchiectasis or extensive lung scarring, has increasingly been recognized as a cause of chronic pneumonia in thin but otherwise healthy postmenopausal women. Tuberculosis should be suspected in persons from endemic areas, the immunocompromised, and those who have served time in prison or been homeless. Patients with AIDS are prone to opportunistic infection with Pneumocystis, Histoplasma, Mycobacterium avium, or Cryptococcus, which tend to present with interstitial infiltrates. They are also highly susceptible to pneumococcal disease; the age-related incidence of pneumococcal pneumonia may be increased 50- to 100-fold in young adults with HIV infection. For this reason, patients with CAP should be asked about HIV risk factors and screened if appropriate.
Clinical Presentation
In younger patients with pneumonia, acute severe malaise and subjective fever are common, often with chills, cough, and sputum production, or at least a sensation of needing to produce sputum. When sputum is produced, it may be flecked with blood. Middle-aged men with underlying lung disease nearly always have increased sputum production. Elderly subjects tend to have much less prominent symptoms; they produce lower levels of cytokines and may respond to them less vigorously than younger adults. A common presentation of pneumonia in older adults is that they are less communicative than usual, or “not acting themselves.” Much has been made of the “classical” presenting symptoms of pneumonia, as described by Osler: the sudden onset of rigors, followed by high fever, cough, pleuritic chest pain, and production of tenacious blood-tinged sputum. This presentation is uncommon today, perhaps because the incidence of CAP in otherwise healthy adults is much lower now than in the preantibiotic era. Diarrhea is common in Legionnaires disease, but it is also frequent in pneumococcal pneumonia, probably as a nonspecific gastrointestinal response to circulating cytokines. Fever, cough, and sputum production without an infiltrate are referred to as acute purulent tracheobronchitis. In those without chronic lung disease, such an illness is generally viral; in a patient who does have such chronic disease, bacterial superinfection, for example, with Haemophilus influenzae, may be responsible. Persistent cough of several weeks’ duration without fever or sputum suggests pertussis or a postviral infection syndrome, for example, due to adenovirus. Several prediction rules for pneumonia exist, but they all have shortcomings and cannot be allowed to replace clinical judgment.
Physical Examination
Younger patients with bacterial or influenza pneumonia appear acutely ill. In contrast, elderly and frail persons may simply seem listless. Young patients nearly always have fever and cough, often with chest pain, whereas these symptoms are often absent in the elderly. Younger adults with viral, Mycoplasma, or Chlamydophila pneumonia generally do not look as acutely ill, and those with tuberculosis or other more chronic forms of pneumonia may appear chronically ill or may look relatively well. Vital signs are of great prognostic importance. Physicians should personally determine the respiratory rate and pay close attention to elevated pulse and respiratory rate or low blood pressure.
In bacterial pneumonia, crackles and increased tactile fremitus are generally present over the affected area. Dullness to percussion is detectable in about one-half of cases. Bronchial breath sounds and egophony strongly suggest pneumonia when present but are not sensitive for diagnosis. The failure to detect excursion of the diaphragm by percussion suggests that an effusion is present. Unfortunately, the overall sensitivity of the physical examination for pneumonia is fairly low, and pneumonia is usually diagnosed not by physical findings but by chest radiograph, with the absence of an infiltrate on a high-quality chest radiograph with posteroanterior and lateral views excluding the diagnosis.
Radiographic Findings
In most cases, the radiographic appearance of a pulmonary infiltrate provides only limited insight into the etiology. Dense consolidation of a segment or lobe is usually bacterial; when due to pneumococcus, such an infiltrate tends to be associated with bacteremia (Figure 189-2).
Figure 189-2
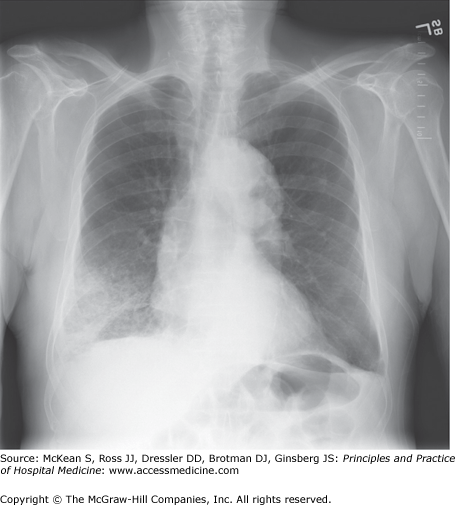
Pneumococcal lobar pneumonia. A 78-year-old man with chronic lung disease had subjective fever, right-sided pleuritic chest pain, and greatly increased shortness of breath for 2 days. He was afebrile, and his WBC count was 10,600 with 40% band forms. Blood cultures were positive for Streptococcus pneumoniae. A sputum submitted for culture more than 24 hours after antibiotics were begun yielded no pneumococci.
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


