TOPICS
1. Hemostasis and cardiac surgery
2. Prevention of blood loss during cardiac surgery
4. Outcomes following transfusion
5. Massive transfusion and cardiac trauma
6. Options for patients who refuse blood product administration
7. The emergency patient from the cardiac catheterization laboratory
Bleeding and the need for blood products frequently complicate both elective and emergency cardiac surgery. Innumerable surgical database analyses undertaken in recent years have demonstrated the deleterious effects of blood and blood component transfusion in cardiac surgery patients. Further complicating medical decision making, there are also data demonstrating the deleterious consequences of the agents designed to minimize the need for those very transfusions. Conversely, there are other studies which highlight the negative effects of failing to transfuse. This chapter will examine the causes, prevention, and management of perioperative bleeding in cardiac surgery. Additionally, since most cardiac surgical emergencies are associated with increased bleeding these too will be reviewed.
HEMOSTASIS AND CARDIAC SURGERY
Hemostasis during and after cardiac surgery begins with surgical control of active bleeding sites. Unfortunately, control of bleeding in cardiac surgery is far more complicated than the mere application of suture to a bleeding vessel. Rather, the effects of hypothermia and hemodilution perturb the entire coagulation system, which balances clot formation and clot degradation. Anticoagulation required for cardiopulmonary bypass (CPB) coupled with the activation of the coagulation, fibrinolytic, and inflammatory systems further disrupts hemostatic mechanisms.1,2
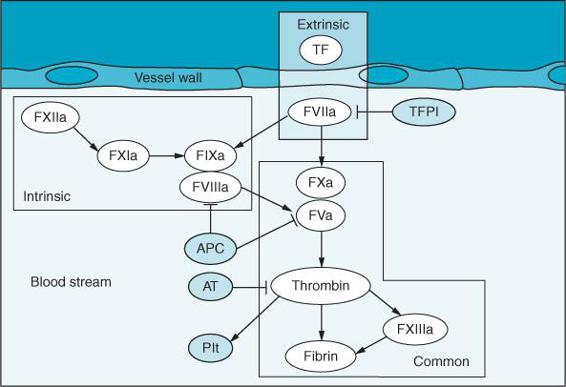
Figure 16–1. The coagulation pathway. The extrinsic pathway consists of tissue factor (TF) and FVIIa. The intrinsic pathway develops from factors FXIIa, FXIa, FIXa, and FVIIIa. The common pathway to fibrin involves FXa, FVa, and thrombin. Factor FXIIIa links fibrin. Thrombin activates platelets (PLT). Regulation of the clotting cascade is provided by tissue factor pathway inhibitor (TFPI) which inhibits the tissue factor VIIa complex. Activated protein C (APC) inactivates factors FVa and FVIIIa. Lastly antithrombin (AT) inhibits thrombin. (Redrawn from: Mackman N. The role of tissue factor and factor VIIa in hemostasis. Anesth Analg. 2009;108(5):1447-1452, with permission.)
Primary hemostasis occurs when the subendothelial layer of a bleeding vessel is exposed to injury. The endothelial cell of the normal vessel wall is antithrombogenic. However, the subendothelial layer is replete with thrombogenic tissue factor (TF) to initiate coagulation (Figure 16–1). Platelets adhere to subendothelial collagen-von Willebrand factor (vWF) via their glycoprotein (GP) Ib receptors to begin the local clot formation. Fibrinogen links adjacent platelets through their GP IIb/IIIa receptors and a clot is born.
Coagulation follows through activation of the well-known coagulation cascades and is limited and regulated by various proteins and mechanisms (Figure 16–2). Tissue factor and factor VIIa through the extrinsic pathway activate factor X leading to the generation of thrombin and then the conversion of fibrinogen to fibrin via the common pathway. The intrinsic pathway follows from the activation of factors XII, IX, and XI and results in activation of factor X and finally generation of thrombin through the common pathway. Various inhibitory proteins moderate the clotting cascade. Tissue factor pathway inhibitor (TFPI) inhibits the initiation of the extrinsic pathway, protein C and protein S inactivate factor VIIIa and factor Va. Antithrombin III (AT III) inhibits thrombin as well as factors IX, XI, XII, and X.
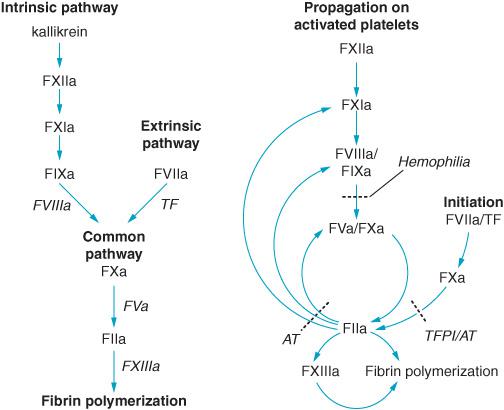
Figure 16–2. A. A simplified, classical approach to the coagulation cascade. B. Propagation of thrombin generation. Initiation of coagulation by the FVIIa/TF complex. Antithrombin (AT) and tissue factor pathway inhibitor (TFPI) regulate thrombin production. Thrombin itself activates factors FXIa, FVIIIa/FIXa, and FVa to further increase thrombin production. (Redrawn from: Tanaka K, Key N, Levy J, et al. Hemostasis and thrombin regulation. Anesth Analg. 2009;108(5):1433-1446, with permission.)
The final phase of normal hemostasis is fibrinolysis. Fibrinolysis involves the production of plasmin through the conversion of plasminogen to plasmin by plasminogen activators. Fibrinolysis remodels the fibrin clot and ultimately leads to the dissolution of the clots.
Manipulation of the normal coagulation system is a critical part of the perioperative management of the heart surgery patient. Complete anticoagulation is required while the patient is on CPB. Likewise, cardiologists frequently employ various degrees of anticoagulation. Patients following percutaneous coronary interventions (PCIs) are frequently treated with abciximab or eptifibatide. These agents antagonize platelet GP IIb/IIIa-mediated binding and prevent platelet aggregation. Often patients presenting for emergency heart surgery in the setting of a failed stent will be treated with these agents and are likely to need platelet transfusion perioperatively. An ever-increasing number of patients are treated with the oral agent clopidogrel, which blocks the platelet’s ADP receptor and likewise inhibits platelet aggregation. Clopidogrel use is ever more increasing as it is taken not only to prevent thrombosis of cardiac stents but for a variety of vascular conditions where antiplatelet activity is desired. Discontinuation of clopidogrel perioperatively carries risk of stent thrombosis and as such perioperative discontinuation of this agent should be at the discretion of the cardiologist and surgeon. However, patients treated with antiplatelet agents are at risk for increased bleeding when taken to heart surgery. Conversely, aspirin has not been shown to increase perioperative bleeding in cardiac surgical patients3 in spite of its antiplatelet effects. Nonetheless, many surgeons will discontinue aspirin use 7 days before surgery.
Heparin is also frequently administered to preoperative cardiac surgical patients at risk for coronary thrombosis. As was discussed in Chapter 4, heparin resistance can occur in patients previously heparinized who are brought to surgery and are required to have an activated clotting time (ACT) of 480 seconds or higher for the initiation of CPB. Reduced concentrations of AT III are associated with prolonged heparin use. Recombinant AT III concentrates and fresh frozen plasma (FFP) can be used to treat heparin resistance secondary to AT III deficiency.
Other patients may come for surgery with various coagulation disorders, platelet deficiencies, hepatic failure, or uremia. All these conditions are likely to impair effective hemostasis following surgery. Consultation with a hematologist is recommended to aid in management of those patients with established clotting disorders.
However, many patients can develop bleeding issues without any history of anti-hemostatic agent drug use or other contributing medical conditions. Cardiac surgery with CPB is associated with a major inflammatory reaction secondary to the contact of blood with the surface of the bypass circuit. Inflammation impairs protein C and protein S regulation of clot formation and increases expression of tissue factor, which can lead to coagulation activation.4 Microvascular thrombosis may occur as a consequence of this inflammatory pathway. Consumption of clotting factors and fibrinolysis can lead to impaired clotting, perioperative bleeding, blood product delivery, and potential morbidity and mortality.
There are many methods employed to monitor the patient’s hemostatic system perioperatively.5 The combination of hemodilution of platelets and clotting factors, factor and platelet activation, and fibrinolysis makes close monitoring of the patient’s coagulation status essential to avoid unnecessary transfusion of allogenic blood products. Traditional laboratory monitors of the coagulation system (eg, prothrombin time, partial thromboplastin time, platelet count, hematocrit, fibrinogen concentration, etc) are usually provided preoperatively and can be ordered intraoperatively as well. However, there is frequently a time delay making such laboratory tests too slow to aid in immediate clinical decision making. Point-of-care measures of coagulation are employed in certain institutions to varying degrees.
When blood contacts the surfaces of the bypass circuit, the coagulation, inflammatory and fibrinolytic pathways are activated. As discussed in Chapter 4 activated clotting time (ACT) and heparin concentration assays are routinely employed to determine a safe degree of anticoagulation status during CPB. Thromboelastography (TEG) permits the diagnosis of various coagulopathic states including factor deficiency, platelet dysfunction, and fibrinolysis. TEG is employed in some institutions to aid in the postoperative management of bleeding through identification of the source of the coagulation deficit.6 Efforts to provide for bedside determination of platelet function and not just platelet count are ongoing through the use of whole blood aggregometry.7
PREVENTION OF BLOOD LOSS DURING CARDIAC SURGERY
Because so many patients present with or develop impaired hemostatic function during cardiac surgery all efforts are undertaken to minimize blood loss. The Society of Thoracic Surgeons has prepared extensive guidelines to promote blood conservation and minimize blood transfusion in the cardiac surgery patient.8 Such interventions include the use of antifibrinolytic agents, preoperative use of recombinant human erythropoietin, maintenance of higher heparin concentrations during longer CPB runs to minimize activation of the hemostatic system, use of red cell salvaging devices for blood conservation where appropriate, use of acute normovolemic hemodilution in stable patients with an adequate hematocrit, preoperative autologous blood donation where indicated, and the use of off-pump techniques if applicable. Each of these efforts is designed to reduce the need for allogenic transfusion of blood products.
The use of antifibrinolytic agents has been at the center of efforts to reduce perioperative blood loss in the cardiac surgery patient. Aminocaproic acid and tranexamic acid are so-called “lysine analogues.”9 These drugs attach to the lysine-binding site of plasminogen and plasmin displacing it from fibrin. Thus, they impair fibrinolysis. Aprotinin is a serine protease inhibitor which prevents plasmin-mediated fibrinolysis and many of the enzymatic intermediaries that contribute to the systemic inflammatory response associated with CPB.10–13
Recent studies have demonstrated that patients treated with aprotinin have an increased incidence of mortality, stroke, and/or renal dysfunction. However, the lysine analogues were not associated with such outcomes.14,15 There are various protocols for administering aminocaproic acid such as 5 to 10 g slow bolus followed by an infusion of 1 g/h up to a total of 15 g. Tranexamic acid is more potent, and is administered as 30 mg/kg loading dose followed by a maintenance infusion of 16 mg/kg/h.15 However, individual institutions often have their own dosing protocols. Because of adverse outcomes studies, aprotinin use has been discontinued. Use of lysine analogues should be jointly undertaken after discussion with the attending surgeon after considering patient morbidities, risks, and benefits, especially in patients with renal impairment.8
WHEN TO TRANSFUSE
There is much variability in cardiac surgery and cardiac anesthesia practice as to when transfusion of blood products is indicated. There is no support for a specific “transfusion trigger”8; however, transfusion for a hemoglobin less than 6 g/dL is considered “reasonable” by the Society of Thoracic Surgeons/Society of Cardiovascular Anesthesiologists guidelines. In determining when to transfuse the risks of anemia must be balanced against the risks associated with blood product administration. Karkouti et al have found that severe anemia during CPB presents an increased risk of renal failure, stroke, and death.16–18 Preoperative anemia has likewise been found to be associated with adverse outcomes in cardiac surgery patients. Moreover, the degree of acute anemia that cardiac surgery patients can tolerate is inversely related to their baseline hemoglobin concentration.19 Indeed, a decrease in baseline hemoglobin concentration greater than 50% was associated with a 50% increase in the composite risk of death, stroke, or renal failure.19 Consequently, the suggested transfusion threshold of hemoglobin 6.0 g/dL may be too low for a person with a baseline Hb concentration of 18 g/dL.
Efforts to establish a physiologic guide to transfusion have also been suggested.20 The oxygen extraction ratio is a measure of global oxygenation. It is a ratio between tissue oxygen delivery and uptake. Transfusion based upon low Hb concentration in patients with a normal oxygen extraction ratio (< 30%) may not be warranted. Additionally, the so-called “storage lesion” of packed cells due to decreased concentrations of 2,3-diphosphoglycerate (DPG) may render transfused cells less useful in delivery of oxygen to the tissues than might otherwise be expected.
Irrespective of what methods are used to determine when to transfuse the cardiac surgical patient, there is no doubt that wide variations in practice patterns exist.21 More than 20% of all blood products given nationally find their way to cardiac surgery patients. However, it is possible to predict which patients will likely require greater than 5 units of RBCs on the day of surgery.22,23 Ultimately, efforts should be undertaken to employ multiple modalities of perioperative blood conservation to reduce the need for allogenic transfusion.24 These modalities include: preoperative autologous blood donation, use of erythropoiesis stimulating agents, antifibrinolytic use intraoperatively, and perhaps intraoperative acute normovolemic hemodilution. Routine use of desmopressin acetate (DDAVP) to promote the release of endogenous factor VIII precursors is not recommended.8
In spite of the desire to minimize blood loss during cardiac surgery, none of the blood conservation methods have been shown to reduce morbidity and mortality.24 Additionally, the recent aprotinin controversy illustrates how efforts to prevent blood loss with this agent had deleterious outcomes. Consequently, the risk of blood conservation techniques in cardiac surgery must be balanced against the risk of transfusion.
OUTCOMES FOLLOWING TRANSFUSION
Should red cell transfusion be considered necessary it is important to note that an increasing number of studies have demonstrated that exposure to even one to two units of red blood cells is associated with decreased survival following cardiac surgery.25 Suggested mechanisms by which red cell transfusion decreases survival include transfusion-related immunosuppression and congestion or damage of the microvascular circulation secondary to the altered morphology of the transfused red blood cells. Blood transfusion has similarly been associated with a reduced quality of life following cardiac surgery.26 Other analyses of large surgical populations associate red blood cell transfusion with increased risk for postoperative atrial fibrillation27 and heart failure.28 Since development of postoperative atrial fibrillation is believed related to an inflammatory mechanism, it is suggested that the modulation of inflammation due to the blood transfusion may contribute to postcardiac surgery atrial fibrillation. Use of statin drugs which have anti-inflammatory effects may decrease the incidence of atrial fibrillation in transfused patients.27 Surgenor et al28 suggest that the increased risk of postoperative low output heart failure following transfusion occurs secondary to a number of possibilities including:
• Increased systemic inflammatory response leading to hypotension requiring various mechanical or inotropic supports
• Packed cell storage lesion whereby decreased 2,3-DPG hinders the unloading of oxygen to the tissue from the red cells
• Pulmonary capillary sludging secondary to the deformed morphology of stored red blood cells leading to impaired capillary transit
The suppression of the immune system associated with blood transfusion was thought by Surgenor et al to more likely manifest in an increased infection risk in transfused patients rather than impact their immediate separation from CPB.
Transfusion of packed cells stored for more than 2 weeks has also been shown to worsen outcomes29 following cardiac surgery. Since the storage lesion of banked blood becomes manifest after 2 weeks, Koch et al suggest that decreased cell deformability can impede microvascular flow. Additionally, the biochemical changes associated with blood stored greater than 2 weeks may likewise contribute to the increased morbidity and mortality associated with transfusion. Transfusion of platelets has not been shown to contribute to postoperative mortality.30
So what to do?? Permitting too low hemoglobin concentration will lead to risks. Administering even one unit of transfused blood likewise carries risk. Certainly, transfusion of red cells should not be automatic or primed to a set transfusion trigger. Each patient should be considered individually and an appropriate plan for blood cell conservation considered if appropriate. Hemodilution from excessive crystalloid fluid administration should be avoided. When to begin transfusion for a particular patient remains problematic, however, measures such as oxygen extraction ratio may provide some additional insights along with clinical signs of inadequate oxygen tissue delivery. What is becoming clear is that red cell transfusion has significant risks well beyond classical transfusion reactions and infection. Thus, both surgeon and anesthesiologist should discuss the risks and benefits of red cell transfusion when considered in each patient perioperatively. Surgical control of active bleeding sites is of course essential in mitigating blood loss perioperatively. Platelet, FFP, and cryoprecipitate transfusion should also be considered when appropriate.
MASSIVE TRANSFUSION AND CARDIAC TRAUMA
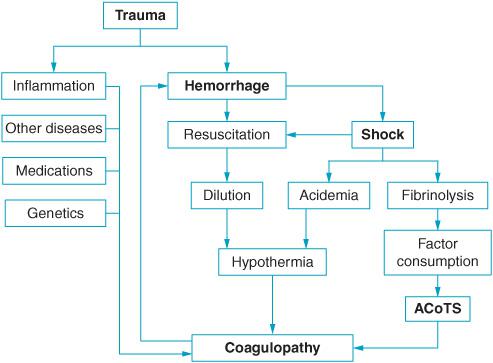
Patients with cardiac trauma can present emergently following penetrating or blunt chest wounds. Often these patients arrive with little additional workup and may have multiple other undetected injuries. Patients generally are brought to the operating room intubated, receiving fluids and blood transfusion through multiple venous lines. Patients frequently are exsanguinated, hypovolemic, hypotensive, and acidotic (Figure 16–3). The surgical team should be assembled to open the sternum immediately upon the induction of anesthesia as such patients generally do not tolerate institution of positive pressure ventilation. If the airway has not already been secured, in-line neck stabilization is often necessary as there may be concomitant neck injury. A video-assisted laryngoscope can be useful in this emergency setting. Arterial pressure monitoring should be established as quickly as possible. Ketamine and muscle relaxants can be employed for rapid sequence induction and endotracheal tube placement. Often these patients will tolerate only very limited amounts of anesthetic agents due to severe hemodynamic instability and as such there is a high risk of awareness in this patient population.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


