Abstract
Hemorrhage is a leading cause of death in trauma, following head injury. Shock is defined by inadequate tissue perfusion with hemodynamic instability and organ dysfunction.1–10 In trauma, the most common cause of shock is due to acute hemorrhage. Advanced Trauma Life Support (ATLS) describes four classes of hemorrhage,1 but these are not relevant to real world practice, due to different injury types (blunt vs. penetrating), age (due to blunted physiologic responses in the elderly), comorbidities, and medication use (beta blockade reduces the chance of tachycardia in response to decreased blood pressure).6–14 Bradycardia may also be seen in hemorrhage, due to several causes including vagal stimulation and failure to mount a tachycardic response.13,14
Introduction
Hemorrhage is a leading cause of death in trauma, following head injury. Shock is defined by inadequate tissue perfusion with hemodynamic instability and organ dysfunction.1–10 In trauma, the most common cause of shock is due to acute hemorrhage. Advanced Trauma Life Support (ATLS) describes four classes of hemorrhage,1 but these are not relevant to real world practice, due to different injury types (blunt vs. penetrating), age (due to blunted physiologic responses in the elderly), comorbidities, and medication use (beta blockade reduces the chance of tachycardia in response to decreased blood pressure).6–14 Bradycardia may also be seen in hemorrhage, due to several causes including vagal stimulation and failure to mount a tachycardic response.13, 14
Management of hemorrhage in trauma requires: (1) hemorrhage control, (2) restoring intravascular volume, (3) delivering adequate oxygen, and (4) maintaining functional blood composition. This chapter will focus on restoring intravascular volume, specifically transfusion. Balanced resuscitation and massive transfusion protocol (MTP) are also key resuscitation components.3–8
Blood Products
A variety of blood products may be provided (Table 3.1). There are several types of blood antigens.
Three primary categories of blood antigens are A, B, and AB. Group O has no antigen type.
Blood type O is the universal donor (due to lack of antigens), while AB+ is the universal recipient.
The Rhesus (Rh) system contains over 50 antigens, with the D antigen the most important (usually specified as + or −).3–8, 15
For non-emergent transfusions, blood is typically typed and crossed. In a massive transfusion protocol, this is not possible. Blood products set aside for a massive transfusion protocol should be checked before trauma.15–18
For male trauma patients, type O+ blood can be provided if the patient’s type is unknown, and for females, type O− blood should be given if the patient’s blood type is unknown.
| Product | Contents | Considerations and Volume | Threshold | Potential Complications |
|---|---|---|---|---|
| Packed red blood cells (pRBCs) | Red blood cells improve oxygen-carrying capacity |
|
| Fluid overload, transfusion reaction, infection, fever, allergy |
| Fresh frozen plasma (FFP) | Contains all clotting factors |
|
| Infection, inflammatory complications |
| Cryoprecipitate | Contains factor VIII, vWF, fibrinogen |
|
| Infection, inflammatory complications |
| Platelets | Apheresis pack is equal to 6 units of non-apheresis packs |
|
| May result in TRALI |
Negatives of Crystalloid Resuscitation
Traditional ATLS teaching is to provide 1–2 L of crystalloid solution, though more recent editions lean away from this.1 Crystalloids in trauma can result in dilutional coagulopathy, impaired oxygen delivery to tissues due to dilutional anemia, hypothermia worsening metabolic acidosis if normal saline is utilized, and clot dislodgement.4, 9, 10
Trauma Coagulopathy and the Lethal Triad
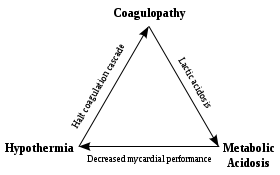
Coagulopathy in severe trauma is associated with increased morbidity, higher transfusion, increased organ dysfunction, and increased mortality. The lethal triad of (1) hypothermia, (2) coagulopathy, and (3) acidosis is classically associated with worse outcomes in trauma (Figure 3.1, Table 3.2). These three factors cause and contribute to further bleeding and coagulopathy.4–10
Coagulopathy occurs in close to 25% of trauma patients due to many causes including: depletion and consumption of clotting factors, platelet dysfunction, increased fibrinolysis, and loss of RBCs.
Resuscitation should focus on restoring the coagulation system, clot strengthening, hemorrhage control, and replace volume with appropriate products.4–10, 19

Figure 3.1 Lethal triad of trauma
| Lethal Triad Factor | Treatment |
|---|---|
| Hypothermia | Warmed fluids and blood products, forced air patient warming device/warm blankets, minimize exposure, increase ambient temperature, continuous monitoring |
| Acidosis | Correct underlying physiology by correcting hemodynamic status, balanced resuscitation, control source of hemorrhage |
| Coagulopathy | Balanced blood product resuscitation, correction of other factors in lethal triad |
Blood product transfusion centers on several aspects. Packed RBCs provide oxygen and nutrients. Other aspects of hemostasis include clot initiation, amplification, and propagation.3–10, 15, 19
Endothelial injury exposes prothrombogenic substances to platelets, forming a loose plug, which acts as a catalyst for coagulation proteins (the coagulation cascade).
Thrombin activates other factors, amplifying thrombin production and activating factor XIII. This forms fibrin cross-links that stabilize the clot. Thrombin also activates a fibrinolytic process that prevents coagulation system overactivity.
Massive hemorrhage is associated with an overwhelmed coagulation system, which is unable to balance between coagulation and fibrinolysis. Traumatic coagulopathy often presents early in resuscitation due to tissue injury, ischemia, clotting factor dilution, hypocalcemia, hypothermia, acidosis, inflammation, and fibrinolysis, independent of clotting factor deficiency.3–7, 19
Damage Control Resuscitation
Damage control resuscitation (DCR) possesses several aspects (Box 3.1). DCR is a systematic approach to trauma management and severe injury, beginning in the ED, through the operating room (OR), and into the intensive care unit (ICU). It aims to maintain intravascular volume, control hemorrhage, and correct the lethal triad. Stages include (1) recognition (often pre-hospital), (2) hemostatic resuscitation, (3) rapid movement to the OR for damage control surgery, and (4) stabilization in the ICU, with reoperation in 24–26 hours.3–10
Damage control surgery focuses on management of the metabolic derangement of ongoing bleed, with abbreviated surgical operations that control hemorrhage and spillage from anatomical areas including the gastrointestinal system. Definitive operation is deferred until the patient is stabilized, targeting normothermia, the use of fewer products, and decreased coagulopathy.3–10
Permissive Hypotension
This is also known as hypotensive resuscitation. The focus is to maintain adequate perfusion while avoiding the disruption of an unstable clot at an injury site.3–10
Penetrating trauma commonly includes a focal site of injury, and preventing clot disruption may improve bleeding control. Cyclic over-resuscitation may lead to rebleeding, worsening hypotension.
Low blood pressure is not the target, as this can worsen organ perfusion. Rather, hemorrhage control is the goal. Once control is achieved, hemodynamic normalization is appropriate.
Controversial: The strategy is largely based on animal studies, with one study being a non-blinded study in 1994.20 There are several interpretations of permissive hypotension goals. Studies have not demonstrated worse outcomes for permissive hypotension in penetrating trauma. It has not demonstrated similar outcomes in blunt trauma, and, in head trauma, permissive hypotension is contraindicated due to the risk of hypotension aggravating secondary injury. This is also dangerous in prolonged transport/retrieval and in patients with chronically elevated hypertension.3–10, 20–22
Permissive hypotension, if followed, should be administered with care. Factors to consider include patient mental status, the likelihood of CNS injury, type of injury, and injury severity (such as ongoing hemorrhage). Delayed fluid resuscitation is likely more harmful unless rapid, emergent surgical exploration with rapid bleeding control is possible.3–10
Minimal Volume Normotension
A more optimal approach is minimal volume normotension, recently advocated in the literature.
A target mean arterial pressure of 65 mm Hg is utilized with a good radial pulse and pulse oximetry waveform, as long as intracranial injury is not suspected and this level allows adequate perfusion. If perfusion is not adequate, a higher target can be used.3–6
Strategy:
MAP <65 mm Hg ➔ Provide balanced blood products
MAP >65 mm Hg ➔ Evaluate perfusion with pulses, lactate, mental status, capillary refill
If MAP >65 mm Hg with perfusion ➔ no action required
If MAP >65 mm Hg with poor perfusion ➔ provide analgesia with fentanyl (doses of 25 mcg IV), which will decrease catecholamine release and allow vasodilation. If MAP decreases <65 mm Hg, then provide balanced resuscitation
Balanced Resuscitation
Balanced resuscitation focuses on reversing traumatic coagulopathy early in resuscitation. This is completed though providing blood products in a close to equal ratio (1:1:1) of packed red blood cells (pRBCs), fresh frozen plasma (FFP), and platelets, avoiding dilution of coagulation factors, which begins in minutes.23–27
Balanced resuscitation includes decreasing traumatic coagulopathy while maintaining or improving end-organ perfusion.
FFP possesses properties and substances that can reduce endovascular leak.
Massive transfusion protocols decrease the incidence of transfusion complications, reduce traumatic coagulopathy, and improve patient outcomes. Massive transfusion entails providing 1:1:1 (pRBCs:FFP:platelets) (Box 3.2).23–27
Balanced resuscitation and MTP should target several parameters, most importantly patient hemodynamic status and hemorrhage control (Box 3.3).
Box 3.2 MTP Definition
Total replacement of >1 blood volume in 24 hours, or
>50% blood volume replacement in 4 hours, or
In children, transfusion of >40 mL/kg
Improvement in hemodynamic status
Hemorrhage control
Temperature >35°C
pH >7.2, base excess <−6, lactate <4 mmol/L
Ionized Ca >0.9–1.1 mmol/L
Hemoglobin: Do not use alone, but only in conjunction with hemodynamic status and other markers
Platelets >50 × 109/L
PT/APTT <1.5× of normal
Fibrinogen >1.0 g/L
Primary Literature for MTP
PROMMTT
Demonstrated 1:1:1 vs. 1:1:2 was associated with improved 6-hour survival after admission.26, 27
PROPPR
Demonstrated 1:1:1 vs. 1:1:2 was associated with no difference in mortality at 24 hours or 30 days, though more patients in the 1:1:1 group achieved hemostasis and experienced fewer deaths due to exsanguination by 24 hours.23
When Should Massive Transfusion Be Activated?
This strategy should be utilized in several circumstances, though a low threshold to activate is advised23, 28–30:
(1) Clinical judgment in the setting of severe trauma with hemorrhage shock.
(2) Clinical scores may be utilized, such as the ABC score.29, 30 A score greater than 2 (points for systolic BP <90 mm Hg in the ED, HR >120 bpm, positive FAST exam, and penetrating mechanism of injury) or with physician judgment/concern for hemorrhage shock due to injury warrants activation of MTP.
Other factors warranting consideration for MTP include uncontrolled bleeding, SBP <110 mm Hg, HR >105 bpm, Hct <32%, pH <7.25, INR >1.4. However, clinical judgment is recommended over use of defined numbers.3–10
How to Run MTP
Multiple points of IV access are advised. pRBCs provide volume and oxygen carrying capacity and are often the first product provided. Platelets should be started at the same time through an additional IV, but platelets cannot be provided through a blood warmer. O− blood should be given for females, O+ blood for males. One pack of apheresis platelets is equivalent to six packs of platelets. These should not be cooled. For plasma, AB plasma is the universal donor. AB and A plasma can be used. Once the patient is hemodynamically stable or bleeding is controlled, massive transfusion can be deescalated.3–10, 31
Cryoprecipitate contains Factor VIII, Von Willebrand factor, and fibrinogen. If the patient continues to bleed with resuscitation or if the massive transfusion is deescalated, check fibrinogen. If fibrinogen is less than 100–150 mg/dL, 10 units of cryoprecipitate should be provided, which raises the fibrinogen by approximately 100.3–8, 32 Calcium supplementation may also be required.
Other Products
Tranexamic Acid (TXA)
TXA is an anti-fibrinolytic that stabilizes the acute clot formed at the site of injury. Several studies, including the MATTERS and CRASH-2 studies, support its use.33–36 Its use is recommended in patients with traumatic hemorrhage receiving blood products as 1 g IV over 15 minutes, followed by 1 g over 8 hours if the patient can receive it within 3 hours post injury. Past 3 hours, TXA may worsen outcomes.33–36
Calcium
Hypocalcemia is common in critically ill patients and trauma. Calcium functions as a cofactor in the coagulation cascade. Citrate, which is an anticoagulant used in blood components, can worsen hypocalcemia through calcium chelation. Ionized calcium less than 0.7 mmol/L can worsen coagulopathy. Calcium should be provided per ionized calcium level, targeting at least levels of 0.9 mmol/L, or with every four units of pRBCs provided.3–10, 37, 38
PCC
Prothrombin complex concentrate (PCC) is a concentrate of factors II, VII, IX, and X. This was initially developed for hemophilia; however, it is beneficial in reversal of warfarin and direct oral anticoagulants.39, 40 PCC can be used for coagulopathy correction in trauma, but it should be used after FFP. Other indications include intracerebral hemorrhage, where volume is limited. If a patient is on oral anticoagulation, PCC is recommended as first line therapy to reverse anticoagulation. Vitamin K with PCC is needed for reversal of vitamin K antagonsists such as warfarin. PCC use in conjunction with FFP to reverse traumatic coagulopathy in patients not on oral anticoagulation may improve reversal and reduce costs, but further study is required.39, 40
Factor VII
Recombinant factor VIIa was developed for hemophilia and congenital factor deficiency. Factor VII functions as a principle trigger for clot formation. However, it should only be used in salvage therapy in hemorrhage shock with continued bleeding. Routine use is not advised, as the medication may worsen outcomes.3–10, 19, 22, 41
Product Guided Resuscitation
Coagulation assessments including PT, INR, and aPTT/PTT may offer prognostic value, but are difficult to use in guiding transfusion. Another tool is thromboelastography (TEG) or rotational thromboelastometry (ROTEM), which can be used to guide product transfusion (Table 3.3 and Figure 3.2).42–46
This assessment evaluates whole blood coagulation, allowing targeted product transfusion.
TEG evaluates clot initiation, clot maximum strength, and clot lysis in a real-time manner. The machine must be calibrated several times per day, and, after blood draw, the sample must be tested within several minutes.42–46
| Value | Description | Measures | Normal | Abnormal | Transfuse |
|---|---|---|---|---|---|
| TEG-ACT | Activated clotting time to initiation of fibrin formation | Intrinsic and extrinsic clotting factors | 80–140 sec | >140 sec | FFP |
| R time | Reaction time to initial fibrin formation | Intrinsic clotting factors | 5–10 min | >10 min | FFP |
| K time | Kinetic time to fibrin cross linkage | Fibrinogen and platelet number | 1–3 min | >3 min | Cryoprecipitate |
| α angle | Angle from baseline to slope of tracing representing clot formation | Fibrinogen and platelet number | 53–72° | <53° | Cryoprecipitate +/− platelets |
| MA | Maximum amplitude of tracing | Platelet number and function | 50–70 mm | <50 mm | Platelets |
| G value | Calculated value of clot strength | Entire coagulation cascade | 5.3–12.4 dynes/cm2 | – | – |
| LY 30 | Clot lysis at 30 min following MA | Fibrinolysis | 0–3% | >3% | Tranexamic acid |

Figure 3.2 TEG representation
Resuscitation Goals
Blood pressure is commonly utilized in resuscitation as a marker of end organ perfusion. However, blood pressure can be falsely reassuring in trauma. Other goals include lactate <2 mmol/L, urinary output >0.5 mL/kg/h, normal base deficit, and normal hemoglobin/hematocrit. Examination markers such as normal mental status (if able to assess), normal capillary refill, and improved perfusion are also valuable to assess. Trends are also important, rather than absolute points in time.3–10, 20 As discussed, hemorrhage control is another goal.
Anticoagulants
The patient with active hemorrhage from trauma and on anticoagulation is challenging. Coumadin (warfarin) is the standard medication for thromboembolic disease and atrial fibrillation. It acts as an inhibitor of vitamin K epoxide reductase, decreasing the synthesis of factors II, VII, IX, and X, as well as anticoagulant proteins C and S. Effect is measured through PT and INR, and the duration of a single dose ranges from 2–5 days.40,48–52
For the patient with active bleeding in trauma, vitamin K 10 mg IV slow infusion should be provided.
For the patient with intravascular loss from bleeding, FFP should be provided at 10–15 mL/kg. One unit of FFP corrects clotting factors by 2.5–5%, and, to improve clotting status, factor levels must reach 10%.
Four factor prothrombin complex concentrate (PCC) provides faster reversal of warfarin, with initial dosing 25–50 IU/kg. PCC can also be prepared and infused faster than FFP, with each 500 unit vial of PCC equivalent to 4 units FFP.4, 48–52
Direct oral anticoagulants (DOAC) are potent inhibitors of coagulation used for venous thromboembolic disease and atrial fibrillation (in those without mechanical valve) (Table 3.4). With DOACs, reversal of anticoagulation is needed in intracranial hemorrhage, hemodynamic instability, and failure to control site of hemorrhage.4, 48–52
Standard coagulation tests such as PT, INR, and aPTT/PTT may be elevated but cannot be relied on to rule out DOAC effect.
MTP should be activated, and, if the patient has taken DOAC outside of 12–14 hours, then the anticoagulant effects have likely worn off.
Reversal requires PCC or several newer, investigational therapies (Table 3.4).
Table 3.4 Direct oral anticoagulant considerations4
| Medication | Rivaroxaban (Xarelto®) | Apixaban (Eliquis®) | Edoxaban (Savaysa®) | Dabigatran (Pradaxa®) |
|---|---|---|---|---|
| Mechanism | Factor Xa inhibitor | Factor IIa inhibitor | ||
| Renal elimination | 66% | 25% | 35% | 80% |
| Reversal agent |
|
| ||
Transfusion Complications
Several complications may arise with transfusion, related to the products and immunomodulating effects (Table 3.5).15, 53–56 Complications of massive transfusion include hypothermia, as one unit of pRBCs can decrease the core temperature by 0.25°C. Acidosis, hyperkalemia, hypocalcemia, and hypothermia are others.15, 53–56
Table 3.5 Transfusion reaction classification15
| Reaction | Pathophysiology | Symptoms | Occurrence (Units Transfused) |
|---|---|---|---|
| Febrile non-hemolytic reaction | Recipient antibodies react with antigens in the product provided and increased cytokines in product | Fever, often low grade, which resolves with acetaminophen | Approximately 1 in 100–500 units transfused |
| Bacterial infection | Products can provide medium for bacterial growth. Risk highest with platelet products | High fever, chills, hypotension, rigor, nausea/vomiting | 1 in 250,000 units transfused |
| Allergic | Exposure to foreign plasma proteins, often in patients with IgA deficiency | Urticaria, pruritis, hypotension, nausea/vomiting, which may meet criteria for anaphylaxis | 1 in 333 units transfused. Anaphylactic reaction in 1 in 20,000 units |
| Acute hemolytic reaction | ABO incompatibility results in immune reaction and destruction of transfused cells | Symptoms of anaphylaxis with hypotension, tachycardia, confusion, arrhythmia, dyspnea, shock, cardiac arrest | 1 per 250,000–600,000 units transfused |
| Transfusion associated acute lung injury (TRALI) | Transfused cytokines and interaction of patient WBC with antibodies in donor | Acute respiratory distress with fever, pulmonary edema, hypotension, with symptoms within 2–6 hours | 1 in 5,000–150,000 units transfused |
| Transfusion associated circulatory overload (TACO) | Edema, dyspnea, orthopnea, hypertension | Volume overload seen in patients with impaired cardiac function | Approximately 1–8 in 100 units transfused, but varies with disease presence and comorbidities |
| Delayed hemolytic reaction | Fever, jaundice, darkened urine, but may have sub-clinical reaction | Patient antibodies to RBC antigens, often in patients with prior transfusion and shortened RBC survival | Unknown |
| Transfusion-associated graft-vs. -host disease (GVHD) | Range of presentations – anaphylaxis to tachycardia, fever, and hypotension. Often fatal | Immunologic attack of transfused cells against recipient, more common in immunosuppressed patients | 1 in 100–1,000 units transfused in patients with cancer |
Controversies – Whole Blood
Whole blood (WB) is currently in use by the military and is FDA approved for administration if collected, tested for transfusion-associated diseases, and stored properly. There are two types: fresh whole blood (FWB) and stored whole blood (SWB). FWB, or a walking blood bank, is stored up to 24 hours after collection at room temperature. If stored and refrigerated within 8 hours of collection, it is known as SWB.57–60 SWB is approved for use in the civilian setting, but only FWB is used in the military. WB is the ultimate physiologic replacement for hemorrhage in trauma, as it contains platelets and is not as diluted as separated blood products.58–61 WB must be ABO-identical if transfused, but low-titer group O WB can be used in emergencies.57, 62 Though WB simplifies transfusion and is likely ideal for resuscitation, further study is required. Future studies will likely result in regular use of SWB.
Key Points
Related posts:






{kind=link}
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


