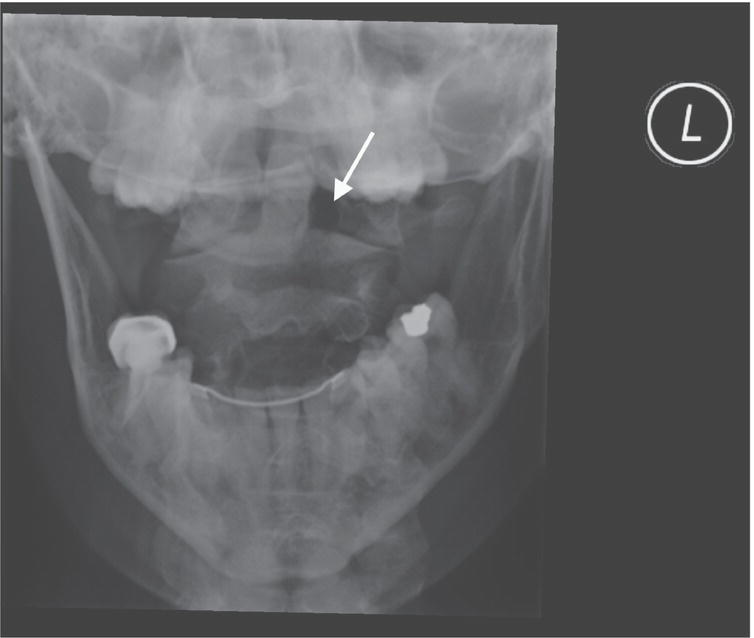
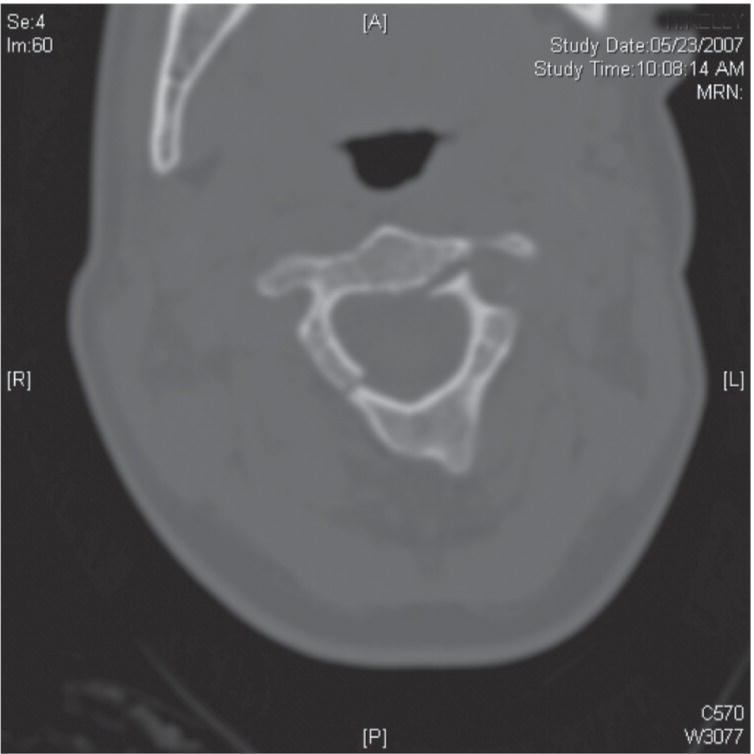
Jesse M. Pines1,2 and Fernanda Bellolio3 1 US Acute Care Solutions, Canton, OH, USA 2 Department of Emergency Medicine, Drexel University, Philadelphia, PA, USA 3 Department of Emergency Medicine, Mayo Clinic, Rochester, MN, USA Of the 138.9 million US emergency department (ED) visits in 2017, 26.2 million – nearly one in five visits were for injury.1 Injured patients commonly undergo assessment for potential injury to the cervical spine (C‐spine), and a subset of patients undergo radiographic imaging (X‐ray or computed tomography [CT]). The diagnostic yield of C‐spine imaging is low and has been estimated at 2–4% of all imaging studies ordered.2,3 As a result, many patients without injuries undergo negative radiographic evaluations. The development of sensitive clinical decision rules to help identify patients who are at extremely low risk of a cervical spine injury (CSI) has been exceptionally useful for clinicians who hope to reduce unnecessary imaging. CSIs also occur, but more rarely in the pediatric blunt trauma population. Their overall prevalence is approximately 1.3%, increasing in a stepwise fashion from 0.4% in infants to 2.6% in adolescents.4 Despite this, C‐spine CT imaging of injured children continues to increase, especially outside of Level I pediatric trauma centers.5 To minimize unnecessary ionizing radiation exposure in children and to ensure the appropriateness of C‐spine imaging while also maximizing patient safety, emergency physicians need to be able to identify a subset of patients at very low risk of clinically significant injury who can have their C‐spines safely cleared without imaging. Older adults (≥65 years of age) with blunt trauma are also commonly evaluated for potential CSIs. Anatomic and physiologic factors associated with these older patients, including osteopenia, osteophytes, and relative immobility, predispose them to CSIs even by low‐impact or minimal‐energy mechanisms. The overall 1‐year mortality for older adults who sustain C‐spine fractures is between 24% and 28%, necessitating that emergency physicians evaluating these patients remain acutely aware of the significance of these injuries in this population.6,7 Two rules have been developed using accepted clinical decision rule methodology: the National Emergency X‐ray Utilization Study (NEXUS) criteria, referred to as the NEXUS low‐risk rules, and the Canadian C‐spine rules (CCR).8,9 Each rule has been derived and validated in large and diverse populations of ED patients with very high sensitivity and negative predictive values (NPVs). There are multiple radiographic modalities available to study the C‐spine, including plain films (Figure 7.1), CT scan (Figure 7.2), and magnetic resonance imaging (MRI). While CT and MRI are more sensitive and accurate for fractures, plain films involve less radiation than CT. However, often plain films are inadequate because of poor patient positioning, patient body habitus, degenerative joint disease, or age‐related changes (such as osteophytes). When the lateral view does not provide an adequate view of the C7–T1 space, repeat films with special (i.e., swimmer’s) views are necessary to definitively rule out injuries. Instead of repeat films, physicians often perform CT scans on patients with inadequate X‐rays. MRI provides additional information over the CT scan in that it can identify ligamentous and spinal cord injuries. Figure 7.1 Open mouth odontoid cervical spine X‐ray showing widening of the lateral pillar (arrow) of the first cervical vertebra, consistent with acute fracture. Figure 7.2 A second vertebral fracture is demonstrated on a cervical spine CT. There is also an open question about what constitutes a “significant” CSI. The two major decision rules for CSIs were derived and validated using plain radiography, which is less sensitive than CT and MRI. Some clinicians may argue that the decision rules may not be sensitive enough and that any C‐spine fracture is important information, because patients with any fracture might be treated differently from those without a fracture through a better understanding of the prognosis, the treatment in terms of immobilization, or the provision of pain control. Examples of clinically insignificant fractures as defined by the derivation and validation studies of the NEXUS and CCR include spinous process fractures, simple wedge fractures without loss of 25% or more of vertebral body height, isolated avulsion fractures without accompanying ligamentous injury, Type 1 odontoid fractures, end plate fractures, fractures of osteophytes, trabecular bone injuries, and transverse process fractures. Finally, additional open questions are whether patients should receive an MRI to rule out ligamentous or spinal cord injury following another normal test (e.g., CT or plain radiography), and whether obtunded trauma patients require MRI imaging after a negative C‐spine CT. Which features of the history and physical exam identify patients at very low risk for clinically significant CSIs who do not need radiography? The NEXUS group used pilot study data and expert consensus to create a clinical decision rule that includes five elements (Table 7.1). The NEXUS criteria were assessed as present, absent, or unable to be assessed. Whenever a component of the NEXUS criteria was not able to be assessed, the patient was considered not to have met that criterion. Patients who met all five criteria were considered to be low risk for clinically significant CSI and to not require any radiography. Table 7.1 NEXUS low‐risk criteria Source: Data from [8]. The initial study for the NEXUS criteria was a prospective observational study at 21 US medical centers that tested the hypothesis that blunt trauma patients who met all of the criteria would have an extremely low probability of CSI. All patients who underwent imaging of the C‐spine were included unless they had penetrating trauma or underwent imaging of the C‐spine for a reason unrelated to trauma. Patients underwent either standard three‐view imaging of the C‐spine (lateral, anteroposterior, and open‐mouth views) or advanced imaging (CT or MRI). The NEXUS criteria were applied in 34,069 patients who underwent imaging of the C‐spine. The prevalence of radiographically documented CSI was 2.4%. Table 7.2 shows the results of the study and the performance of the NEXUS criteria. The criteria from this study missed a total of eight patients with documented CSIs. Only two of those injuries were clinically significant as defined by the study; however, neither required surgical intervention or had any long‐term clinical consequences. With 100% sensitivity and a 100% NPV, it was felt that patients meeting all of the criteria could safely be considered at extremely low risk for CSI and did not need imaging. Table 7.2 NEXUS low‐risk criteria study results and test performance Source: Data from [8]. In a similar study performed at approximately the same time in Canada, Stiell et al.9 created the CCR. This decision rule was first published as a derivation study in 2001. Their goal was similar to that of the NEXUS investigators: to develop a prediction rule with extremely high sensitivity for detecting acute CSIs in stable ED patients with blunt trauma. The authors conducted a prospective cohort study in 10 Canadian EDs and derived the clinical and historical factors that would optimize the detection of a CSI. In this, they differed from the NEXUS investigators, in that the NEXUS criteria did not consider the events surrounding the injury. Patients with blunt head or neck trauma were included in the study if they were alert (defined as a Glasgow coma scale (GCS) score of 15) and stable (defined as a systolic blood pressure >90 mmHg and a respiratory rate greater than 10 but less than 24 breaths per minute). Patients were excluded if they met one of the following predefined criteria: age younger than 16 years, minor injuries not including blunt head or neck trauma (such as lacerations or abrasions), GCS <15, grossly abnormal vital signs, time since injury of greater than 48 hours, penetrating trauma, acute paralysis, known vertebral disease, return for reassessment of the same injury, or pregnancy. Data were collected on 20 standardized clinical findings from the neurologic status, history, and physical exam. Patients underwent imaging of the C‐spine at the discretion of the treating physician. Imaging of the C‐spine was not mandatory; therefore, some patients did not undergo imaging. For those patients without C‐spine imaging, a structured telephone follow‐up was conducted to assess for missed injuries. The purpose of this hybridized criterion standard was to ensure that there were no missed injuries in patients who did not receive radiographs. Patients were considered not to have had a clinically significant CSI if, during the telephone interview at 14 days, they met all of the following criteria: (i) neck pain rated as mild or none, (ii) restriction of neck movement rated as mild or none, (iii) use of a cervical collar not required, and (iv) neck injury did not prevent return of patient to usual occupational activities. The CCR include three sets of criteria that need to be evaluated in a stepwise manner. However, if a patient satisfies all of the criteria, the decision rule indicates a low risk of CSI, and radiography can be avoided. Table 7.3 lists the criteria that must be fulfilled to safely avoid imaging according to the CCR. For the derivation study, a total of 12,782 patients were eligible for the study; of those, 3281 patients were not enrolled and another 577 patients were excluded because they did not undergo imaging and could not be reached for follow‐up. A total of 8924 patients were included in the final study group and had either radiographic imaging or the proxy 14‐day telephone follow‐up. The prevalence of documented CSI in the study was 2%. Table 7.4 shows the study results and test performance. The stepwise nature of the CCR makes it more complicated than the NEXUS criteria and more difficult to remember; however, studies have shown that the rule can be used by paramedics in the field.10 Table 7.3 The Canadian C‐spine rules Source: Adapted from [9]. If yes to any of these, radiographic imaging is recommended. If no, criteria 2 and 3 are assessed. Table 7.4 Canadian C‐spine rules study results and test performance Source: Data from [9]. Stiell et al.11 also compared both sets of rules in a large prospective study in the same EDs that participated in the derivation study for the CCR. The study aimed to compare the performances of the two rules (CCR versus NEXUS) to determine which was more specific, and also to validate the CCR. The methodologies for applying the clinical decision rules were the same as outlined in the original studies, but the inclusion and exclusion criteria of the CCR derivation study were used and not all patients underwent imaging (consistent with the CCR study but in contrast to the NEXUS study). Criteria for both sets of rules were prospectively determined and recorded prior to C‐spine imaging. The authors achieved their objective of validating the CCR. Among the 8283 patients enrolled, 7438 had complete data from both sets of rules and underwent either C‐spine imaging or the 14‐day telephone proxy instrument. The incidence of CSI in this study was 2%. Table 7.5 shows the test results and test characteristics. In comparing the performances of the NEXUS and the CCR, the authors found the CCR to have a higher sensitivity, NPV, and specificity. Table 7.6 shows the results and performances of the NEXUS criteria. Table 7.5 Validation results of the Canadian C‐spine rule and test performance Source: Data from [11]. Table 7.6 NEXUS low‐risk criteria test performance Source: Data from [11]. Finally, in a study that assessed the effectiveness of a strategy to implement the CCR in multiple EDs using a matched‐pair clustered‐randomized design in 11,824 patients in 12 Canadian hospitals, patients seen at intervention sites had a relative reduction in C‐spine imaging of 12.8% (confidence interval [CI] 9–16%; 61.7% versus 53.3%; p = 0.01), and the control group had a relative increase of 12.5% (CI 7–18%; 52.8% versus 58.9%; p = 0.03).12 In addition, the changes were significant when both groups were compared directly: there were no missed fractures and no adverse outcomes in either group. The authors concluded that implementation of the CCR could lead to a significant decrease in imaging without missing injuries. A systematic review compared the accuracy of the CCR and NEXUS criteria. Fifteen studies comprising 79,526 patients were included. CCR had a sensitivity between 90% and 100% and a specificity between 1% and 77%. Median LR− was 0.18 (interquartile range [IQR
Chapter 7
Cervical Spine Fractures
Background
Clinical question
Assessment result for any cervical spine injury
Decision rule
Positive
Negative
Totals
Positive
810
28,950
29,760
Negative
8
4301
4309
Totals
818
33,251
34,069
Sensitivity (CI)
99% (98–100%)
Specificity (CI)
13% (13–13%)
Positive likelihood ratio (LR+)
1.1
Negative likelihood ratio (LR−)
0.08
Clinically significant cervical spine injury
Decision rule
Positive
Negative
Totals
Positive
576
29,184
29,760
Negative
2
4307
4309
Totals
578
33,491
34,069
Sensitivity (CI)
100% (99–100%)
Specificity (CI)
13% (13–13%)
Positive likelihood ratio (LR+)
1.1
Negative likelihood ratio (LR−)
0.03
Radiographically documented injury
Decision rule
Positive
Negative
Totals
Positive
151
5041
5192
Negative
0
3732
3732
Totals
151
8773
8924
Sensitivity (CI)
100% (98–100%)
Specificity (CI)
43% (40–44%)
Positive likelihood ratio (LR+)
1.8
Negative likelihood ratio (LR−)
0
Radiographically documented injury
Decision rule
Positive
Negative
Totals
Positive
161
3995
4156
Negative
1
3281
3282
Totals
162
7276
7438
Sensitivity (CI)
99% (96–100%)
Specificity (CI)
45% (44–46%)
Positive likelihood ratio (LR+)
1.8
Negative likelihood ratio (LR−)
0.01
Radiographically documented injury
Decision rule
Positive
Negative
Totals
Positive
147
4599
4746
Negative
15
2677
2692
Totals
162
7276
7438
Sensitivity (CI)
91% (85–94%)
Specificity (CI)
37% (36–38%)
Positive likelihood ratio (LR+)
1.4
Negative likelihood ratio (LR−)
0.24
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


