FIG. 37.1 Airplane splint. (From Coppard BM, Lohman H: Introduction to splinting: a clinical-reasoning and problem solving approach, ed 2, St. Louis, MO, 2001, Elsevier.)
Positioning
After the initial assessment of the patient is complete, attention is turned to positioning. Proper body alignment is important for orthopedic patients and requires a sound knowledge of operative procedure and body mechanics. Individual surgeons typically have specific preferences for positioning, but general guidelines apply to all patients. The goal is optimal comfort and safety for the operated limb or area. The upper extremities are generally held close to the body, and elevation should be achieved without undue pressure on the elbow or shoulder. The lower extremities are typically placed in a neutral position with support provided for the entire limb, placing heels off the bed.
Elevation of operative limbs is usually indicated to increase venous return, reduce swelling, and promote comfort. In the elevation of a hand or arm, the hand must be higher than the heart with no pressure on the elbow. This position can be achieved with the use of pillows, a sling, or a stockinette device.
Lower extremity elevation is most effective if the toes are above the heart. If the limb is not in an immobilization device, it is kept in a position of extension. This position is achieved by elevating the foot of the bed rather than with the use of pillows. The entire length of the limb should be supported if pillows are used with heels kept off the bed.
Shoulder immobilization can be accomplished with a sling or shoulder immobilizer. An airplane splint (a padded and Velcro shoulder orthotic used to position the shoulder in various degrees of abduction; Fig. 37.1) may be applied for rotator cuff repairs, involved humerus fracture repairs, and postoperative shoulder or arm surgery where shoulder position and elbow flexion control are desired. If a sling is used, the patient is instructed to keep the arm close to the chest with the wrist and elbow supported. All shoulder immobilizers require special care and padding to areas where skin contacts skin.
The approaches for total hip arthroplasty vary in the invasiveness of the hip musculature: (a) the posterior approach, (b) the lateral or transgluteal approach, (c) the anterolateral approach, and (d) the anterior approach.
A. The posterior approach (i.e., Kocher-Langenbeck approach) splits the gluteus maximus muscle and detaches the posterior external rotator muscles (i.e., the piriformis, obturator internus and externus, superior and inferior gemellus).
B. The lateral or transgluteal approach (i.e., Harding approach) splits the gluteus medius muscle and detaches the gluteus minimus and the anterior third of the gluteus medius muscles from the femur.
C. The anterolateral approach (i.e., Watson-Jones approach) is performed posterior to the tensor fascia lata and anterior to the gluteus medius and splits the hip deltoid muscle, which consists of the gluteus maximus and tensor fascia lata muscles.
D. The anterior approach (i.e., short Smith-Petersen and Hueter approach) does not split or detach muscles. This approach is performed over the tensor fascia lata, inside the tensor sheath, anterior and medial to the tensor fascia lata, and lateral to the sartorius and rectus femoris muscles.

From Munro CA: The perioperative nurse’s role in table-enhanced anterior total hip arthroplasty, AORN J 90:54, 2009. Illustration by Kurt Jones.
The patient with a hip pinning is positioned with proper body alignment, and the legs are in a proper neutral position. Care is given to avoid stress to the operative area with exaggerated flexion or rotation. A pillow is placed between the knees during turning to prevent adduction and rotation.
Surgery technique and surgeon preference will determine the appropriate position of postoperative hip patients. For the patient with a posterior or lateral total hip replacement, proper body alignment can be achieved with placement of an abduction pillow between the knees. Most important with these patients is to avoid flexion and adduction of the newly placed joint. There are four basic positions to be avoided after hip surgery: (1) no flexion of the hip past 90 degrees with respect to the axis of the body; (2) no abduction of the leg past the midline of the body; (3) no combined extension of the hip joint with external rotation of the lower extremity; and (4) no flexion with internal rotation. Use of the abduction pillow helps to prevent the patient from getting into positions that could cause dislocation. The patient who has had an anterior total hip replacement, which is a minimally invasive procedure, does not normally require dislocation precautions. Therefore, there is usually no need for an abduction pillow, traction sling, or hip cushion to assist with positioning.2 See Box 37.1 for various surgical approaches.
The perianesthesia nurse should also be familiar with various types of orthopedic equipment that may be used that can affect positioning. At times, patients with total knee replacement and those with more extensive knee arthrotomy are placed in a continuous passive motion (CPM) machine. The purpose of CPM is to enhance the healing process by providing CPM to the joint, thus increasing circulation and movement. However, evidence is showing that the inconvenience and expense may not outweigh the benefit of CPM.3 See further discussion in the section Perianesthesia Care After Knee Surgery.
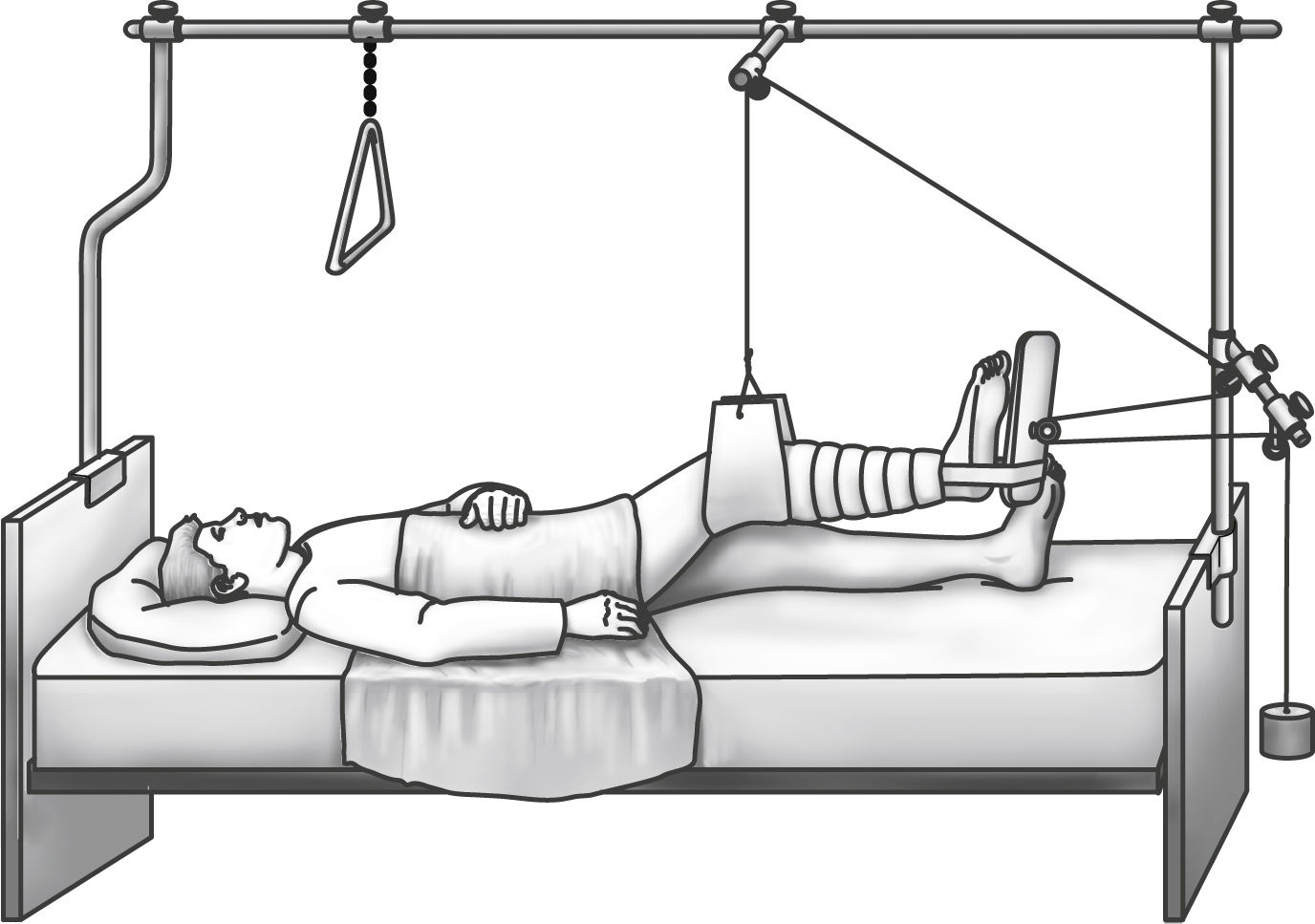
Traction may also be used with various patients to immobilize and align a specific area. The perianesthesia nurse is not usually involved in setting up the traction but should be aware of some basic principles for maintenance: (1) the traction must be continuous, (2) the patient is centered in bed in good alignment to maintain the line of pull in line with the long bone, (3) weights should hang freely and not rest on the floor or bed, and (4) the pulley ropes should be in alignment and free of knots. One type of traction is depicted in Fig. 37.2.
Neurovascular Assessment
Critical to the care of the patient for orthopedic surgery is assessment of the operative limb’s neurovascular status. Nerve compression or any alteration in blood flow to the extremity requires immediate intervention. Assessment is recommended every 15 to 30 minutes because problems can occur within 2 to 4 hours. Baseline neurovascular indicators should be noted from preoperative assessment and from the admission nursing assessment to the postanesthesia care unit (PACU). These indicators can be used to establish any deleterious effects from the surgery and to avoid the masking of potential complications. Both the affected and unaffected limbs are assessed.4
The hallmarks of neurovascular changes from constriction and circulatory embarrassment are pain, discoloration (skin that is pale or bluish), decreased mobility, coldness, diminished or absent pulses, altered capillary refilling, decreased sensation, and swelling (Box 37.2). Pain is common with patients for orthopedic surgery, and the approach to treatment must be individualized. Pain unrelieved with conventional methods, such as elevation, repositioning, and the administration of opioids, must be assessed further. Color indicates circulatory compromise.4 Cyanosis suggests venous obstruction; pallor suggests arterial obstruction. Mobility is assessed by determining the range of motion of the fingers or toes and strongly indicates neural compromise. Fingers are flexed, extended, spread, and wiggled. Toes should be dorsiflexed, plantarflexed, and wiggled. An inability to move the fingers or toes, pain on extension of the hand or foot, or coldness of the extremity is indicative of ischemia. Sensation is described as normal, hypesthetic (dulled), paresthetic, or anesthetic. Alteration in sensation suggests nerve compression or circulatory compromise. Limb perfusion is further assessed with the presence of peripheral pulses and capillary refilling. Capillary refilling is assessed with compression of the nail bed, which causes blanching; when the compression is released, color briskly returns. Compromise delays the filling time. With the development of pulse oximetry, a more reliable method of perfusion assessment is available. With placement of the oximeter sensor on a finger or toe of the affected limb, the pulsation is sensed and oxygen saturation is displayed. This method is more reflective of perfusion than capillary refilling and is valuable when pulses cannot be assessed because of the presence of a cast or dressing.
Care of Immobilization Devices (Cast Care)
Immediate postoperative assessment of the patient after orthopedic surgery should include the type of immobilization device applied. The soft knee immobilizer should be checked for proper placement and closure, and the surgical dressing should be checked for drainage. For care that involves traction, refer to the previous section in this chapter on positioning.
The cast is a rigid immobilization device molded to the contours of the part to which it is applied. The cast has a dual purpose: immobilization in a specific position and provision of uniform pressure on the encased soft tissue. The cast should be inspected for visibility of fingers and toes, enabling neurovascular assessment. If the cast is bivalved, the edges should be inspected for roughness to avoid discomfort and potential skin breakdown. When the patient arrives in PACU, the cast may still be wet, and, if so, special care must be taken to prevent indentations (such as using the palms of the hand to avoid pressure from fingertips). The cast should be supported on a pillow, and hard flat surfaces should be avoided. Improper handling and flat surfaces can cause indentations that can lead to the development of pressure sores. More frequently, a fiberglass cast is applied with quicker drying properties, but the same general principles still apply.4 In general, a full cast may not be placed on a patient where wound drainage is expected (a temporary splint or cast would be used), but any drainage noted on the cast should be circled, and the time should be noted. This documentation can provide a guide for postoperative blood and fluid loss and can alert the nurse if the drainage appears to be excessive.
Wound and Drain Care
All surgical dressings should be checked for drainage and closure. Orthopedic wounds tend to ooze and may bleed more than other surgical wounds, and documentation and notation of drainage on the dressing is recommended to note the amount of drainage. Patients with orthopedic surgery are highly susceptible to infection; therefore, strict asepsis is required when changing dressings or handling drains. Drains may be placed in the wound to minimize blood accumulation and the possibility of infection. If a drain is present, it should be checked to ensure that it is activated, or it may be connected to a vacuum blood tube. Drains should be checked every 1 or 2 hours to maintain a proper suction, and the output should be recorded on the intake and output records.
A patient with total joint replacement may commonly have a large amount of blood loss in the immediate postoperative period. The total perioperative blood loss in hip arthroplasty is typically over 200 mL.5 Blood loss can be significant with all major orthopedic surgeries, but with advances in technology and the implementation of minimally invasive techniques, attempts are being made to keep blood loss at a minimum. Autotransfusion may be used in the form of cell saver in the operating room (OR). Autotransfusion is accomplished with the use of self-contained disposable systems designed for easy setup and safe use. The retrieval of this blood for reinfusion (autotransfusion), in addition to new medical management, has substantially reduced the need for homologous or autologous transfusions. Additionally, an antifibrinolytic agent, such as tranexamic acid, is one emerging medication used to reduce blood loss in orthopedic surgeries.5 Regardless of blood-conserving techniques used, if the patient experiences excessive amounts of blood loss in the PACU, surgeon notification is recommended.
Range-of-Motion Exercises
Range-of-motion exercises can be initiated in PACU as soon as the patient is alert and cooperative. Flexion, extension, and rotation of joints distal to the operative area assist in stimulating circulation and strengthening muscles. Quad- tightening exercises, if permitted by the physician, may also be helpful. Prevention of venous stasis decreases the incidence rate of thromboembolism, and early movement of joints promotes healing and stabilization.
Observation for Complications
Postoperative complications for the patient after orthopedic surgery include deep vein thrombosis (DVT), pulmonary embolism (PE), fat embolism syndrome, compartment syndrome, shock, and urinary retention.
Deep Vein Thrombosis
Prevention of DVT is a major concern for patients undergoing orthopedic surgery, especially total joint replacement.6 Other contributing risk factors include age, previous history of DVT or PE, malignancy, smoking, estrogen or current pregnancy, vein disease, obesity, and clotting disorders.7,8 Thrombosis is the formation of a blood clot associated with three conditions outlined by Virchow in 1846: venous stasis, altered clotting mechanism, and altered vessel wall integrity.9 In reports of total hip arthroplasty before routine prophylaxis, venous thrombosis occurred after total hip replacement in 40% to 80% of patients, and fatal pulmonary emboli occurred in 2%.6 Immobilization impairs the leg muscle action needed to move the blood sufficiently, and the surgical procedure injures vessel walls that activate and alter clotting mechanisms, placing the orthopedic patient at high risk of the formation of a thrombus within the deep vein. An inflammation process begins within the vessel wall and leads to DVT, and the patient usually has pain and tenderness. Signs include swelling and sometimes localized redness. Palpation of the calf reveals firmness or tension of the muscle. A positive Homans sign may be seen, although a positive sign does not accurately diagnose a DVT alone.10 DVT can be difficult to diagnose. Diagnostic tests such as venography, magnetic resonance imaging, or Doppler ultrasound may be indicated.
Prevention of DVT for postoperative orthopedic patients includes providing adequate hydration, early mobility, range-of-motion exercises, mechanical prophylaxis, and pharmacologic prophylaxis when necessary. Mechanical prophylaxis includes antiembolic stockings and external compression devices such as sequential compression devices that enhance venous flow. Surgeon’s preference typically dictates the choice of postoperative anticoagulant therapy, and rehabilitation and mobility beginning the day of or first day after surgery will also help to prevent venous complications.
The ideal thromboembolic prophylaxis regimen for prevention of DVT and PE varies but is not short of recommendations. Some hospitals use a detailed DVT prophylaxis screening tool or protocol to assess each patient’s individual need for anticoagulation therapy and thromboprophylaxis. The American College of Chest Physicians and the American Academy of Orthopaedic Surgeons have made recommendations for VTE prophylaxis.6 Additionally, all health care facilities accredited by The Joint Commission must comply with National Patient Safety Goal 03.05.01 to “reduce the likelihood of patient harm associated with the use of anticoagulant therapy.”1
Pulmonary Embolism
The most serious sequela of DVT is a PE. Symptoms can be minimal if the clot is small to a myriad that may include—with increasing severity—anxiety, dyspnea, tachypnea, hemoptysis, substernal pain, stabbing pleuritic pain, tachycardia, cough, signs and symptoms of cerebral ischemia, fever, elevated sedimentation rate, shock, and sudden death. Immediate nursing care involves administration of oxygen and preparation for possible diagnostic tests (such as chest x-ray) as well as preparation for possible intubation. Medications usually include heparin-bolus doses with continuous infusion or other antithrombolytic agents. Perianesthesia nurses must be vigilant to assess all postop orthopedic patients for signs and symptoms of DVT and PE.
Fat Embolism Syndrome
Fat embolism syndrome is a condition that leads to respiratory insufficiency and is related to multiple fractures, especially of the long bones. It is caused by fat droplets released into the circulation from the bone marrow and local tissue trauma. Similar to PE, these fat globules migrate to the lungs where they cause occlusions. The fat globules break down into acids that irritate vascular walls and cause extrusion of fluids into the alveoli. The lung involvement alters ventilation and leads to hypoxemia. Fat embolism syndrome can lead to adult respiratory distress syndrome. The symptoms related to lung involvement include tachypnea, tachycardia, anxiety, chest discomfort, petechiae over the chest, PO2 less than 60 mm Hg, fever, pallor, and confusion.11 Brain involvement is evidenced by agitation, confusion, delirium, and coma. Immediate nursing care of this sometimes-fatal complication includes administering oxygen, keeping the patient quiet, and preventing motion at the fracture site. Prompt ventilation-perfusion scans may be warranted.
Compartment Syndrome
Compartment syndrome is a condition in which increased pressure within a muscle compartment causes circulatory compromise and leads to tissue necrosis and diminished function of the limb. Left undetected, the compression may cause permanent damage to the extremity. The compartment is described as a fascial sheath that encloses bone, muscle, nerves, blood vessels, and soft tissue. The two main causes of increased pressure to this space are (1) constriction from the outside, such as a cast or bandage that decreases the size of the compartment, or (2) increased pressure within the compartment such as swelling. The hallmark symptoms of compartment syndrome include intense pain unrelieved with conventional methods, paresthesia, and sharp pain on passive stretching of the middle finger of the affected arm or the large toe of the affected leg. The most significant sign is pain out of proportion to that expected with the injury or surgery.6 Progressive symptoms include decreased strength, decreased sensation (numbness and tingling), and decreased capillary refilling; peripheral pulses are not generally compromised. Immediate intervention includes elevation of the extremity, application of ice, and release of restrictive dressings. Compartmental pressures may be determined by the surgeon. If compartmental pressures are greater than 30 mm Hg in the presence of clinical findings, immediate fasciotomy is indicated. Ambiguous readings require continuous monitoring and continued clinical examinations (Fig. 37.3).6 Fasciotomy may be required within 4 to 6 hours of onset of symptoms if conservative measures are unsuccessful.

FIG. 37.3 Synthes (West Chester, PA) hand-held compartment pressure monitor. (From Canale ST, Beaty JH: Campbell’s operative orthopedics, ed 12, Philadelphia, PA, 2013, Elsevier.)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


