FIG. 41.1A, Types of large-diameter catheters. 1. Conical tip urethral catheter, one eye. 2. Robinson urethral catheter. 3. Whistle-tip urethral catheter. 4. Coudé hollow olive-tip catheter. 5. Malecot self-retaining, four-wing urethral catheter. 6. Malecot self-retaining, two-wing catheter. 7. Pezzer self-retaining drain, open-end head, used for cystotomy drainage. 8. Foley-type balloon catheter, one limb of distal end for balloon inflation (i), one for drainage (ii). 9. Foley-type, three-way balloon catheter, one limb of distal end for balloon inflation (i), one for drainage (ii), and one to infuse irrigating solution to prevent clot retention within the bladder (iii).B, Straight catheter. (A, From Wein AJ: Campbell-Walsh urology, ed 9, Philadelphia, PA, 2007, Elsevier; B, From Potter PA, Perry AG, Stockert PA, et al: Fundamentals of nursing, ed 9, St. Louis, MO, 2017, Elsevier.)
The catheter should be anchored securely to the patient’s thigh with a leg strap and locking device with the tubing brought over the leg. The catheter should be secured to prevent undue tension on the urinary meatus. The connecting tubing should be attached to the bed linens so that no proximal loops of tubing lie below the distal tubing; this is a straight gravity drainage system. The tubing should never be under the patient because compression of the tubing obstructs the flow of urine. The tubing should be checked frequently for kinks. The urine receptacle should always be kept below the bladder level to prevent urine reflux up the tubing. Particular attention must be paid to this principle during the transfer of patients.
For collection of a urine specimen from the closed system, a sterile syringe and needle are used. Some catheters have a small specially constructed port from which to draw specimens. On those catheters that do not have such a port, the distal part of the catheter, close to the drainage tube, is used. The area is cleansed with povidone-iodine (Betadine)—provided the patient is not allergic; otherwise the surgeon is consulted for another choice—the needle inserted, and a specimen withdrawn.
Mucus, blood, or both can clog the tubing and prevent urine flow. Irrigations should be administered only according to the surgeon’s orders. All irrigations are sterile procedures and can be either continuous or intermittent. For intermittent irrigation, a large sterile Toomey syringe and sterile irrigating solution (usually normal saline solution alone or with a selected antibiotic) are used. Care must be taken to keep all parts of the drainage system sterile. This action may be accomplished by placing a small sterile plastic cover on the drainage tubing while the irrigation is performed. Irrigations should never be given with pressure. When the bladder is irrigated, no more than 30 mL should be instilled at one time unless ordered otherwise by the surgeon.2,9
After transurethral resection of the prostate (TURP), continuous irrigation is usually preferred. With continuous irrigation, normal saline solution is typically connected with a three-way urinary catheter. Nursing care should include vigilant monitoring of patients for hyponatremia and the development of TURP syndrome.11 The report from the perioperative nurse should include the amount of intraoperative irrigation and the duration of the procedure.12 During the immediate postanesthesia phase, patient confusion should be monitored and differentiated from confusion resulting from amnesiacs, opioids, or hyponatremia (see also the Prostatic Surgery section in this chapter).10,11
If hyponatremia is diagnosed, treatment may include the administration of hypertonic saline solution for a gradual increase in the patient’s serum sodium level. Care includes monitoring for signs of intracellular to extracellular fluid shifts. As fluid moves back into the extracellular space, pulmonary edema and heart failure can occur quickly.11
Suprapubic Catheters
At the completion of a urologic procedure, a suprapubic catheter may be used to drain residual urine from the bladder. A temporary catheter can be placed into the urinary bladder via a stab wound through the lower abdomen and into the anterior bladder wall. The catheter is sutured in place, and a dressing is applied (usually a type of dressing that allows direct observation of the puncture site). The catheter is connected to a straight gravitational drainage system. Care of the suprapubic catheter is similar to that of the urinary catheter. The catheter should be taped securely with a loop made to prevent tension on the bladder wall or the abdomen. The skin around the puncture site should be kept clean and dry. The catheter tubing should be checked periodically for kinks and to ensure that the stopcock valve is open to allow the urine to drain from the bladder.
A suprapubic catheter can also be placed into the urinary bladder via abdominal incision and cystostomy.2 This procedure is typically done for more permanent or long-term use of the suprapubic catheter. The surgeon may choose this method if conventional methods of treatment for urinary incontinence fail, as with spinal cord injury or neurogenic bladder. The care of the catheter is the same as with the puncture wound, but the nurse should also apply nursing care that relates to the abdominal incision.11,12
Ureteral Catheters and Stents
Ureteral catheters are used to drain urine or splint the ureters while they heal.13,14 Ureteral catheters may be used when there is a greater risk of occlusion of the ureter as with stones. In the event of a ureteral injury or surgery around the ureter that may result in significant swelling/inflammation postoperatively, a ureteral stent is used to ensure the ureter remains open. The stent may remain in place for several weeks postoperatively and removed in the urologist’s office. In the case of a more extensive injury, ureteral reimplantation is done laparoscopically (with or without the assistance of the robot) or via laparotomy. The approach taken will depend on the specific location of the injury and laparoscopic skill of the surgeon. Reimplantation may require the ureteral stent remain in place for a longer period of time. The catheters can be placed through the urethra (during cystoscopy) or through abdominal or flank incisions.13,14 Care of ureteral catheters is essentially the same as that for urethral catheters. Attention to patency must be especially meticulous because the renal pelvis can hold only 5 mL without overdistention and damage to the kidneys.13,14
Sterile irrigations are undertaken only as ordered by the physician. Only 5 mL of fluid should be used for the irrigation via gravitational flow. Irrigations should never be given with pressure such as with a syringe and plunger. The nursing staff must be sure to avoid situations that can cause dislodgment or displacement of these catheters or stents, which could be disastrous to the outcome of the surgery. Special care must be taken during patient transfer to ensure that catheters or stents stay in place. One person should be assigned this responsibility during the transfer. If the catheters or stents become dislodged despite all the precautions taken, the surgeon must be notified immediately.13,14
Intake
Optimal fluid intake is exceptionally important for the patient after surgery; increased fluids are the general rule. Fluids should be given orally if the patient can tolerate this preferred route, and intake should be increased to total of 3000 mL in a 24-hour period. Special consideration regarding type and amount of fluids should be taken with any patient with renal insufficiency. Parenteral fluid therapy is indicated for a short time until the effects of anesthesia have passed and is continued only if the oral route of intake is inadequate.10
Dressings
Care of dressings varies according to the procedure and can include anything from a bulky dressing to Steri-Strips or bandages. Many patients are allergic to latex or adhesives, and this must be taken into account when dressings are used.12 Dressings applied after urinary tract surgery often become soaked with blood and urine. They should be reinforced as necessary, and the surrounding skin should be kept clean and dry to prevent unnecessary excoriation and breakdown.10 (Excessive staining that is unexpected for a particular procedure and indicates a complication is so indicated in the discussion of the specific procedure later in this chapter.) Excessive bleeding and hemorrhage are ever-present dangers of this surgery because the kidneys and prostatic bed are extremely vascular. Vital signs must be monitored closely, and all avenues of output, especially the incisions and drainage tubes, should be evaluated frequently for bleeding.9,10
Abdominal Distention
All patients should be assessed for abdominal distention after surgery that involves abdominal and flank incisions (see Chapter 40 for care of the patient after an abdominal incision because the same care applies after genitourinary surgery). These patients can arrive with nasogastric tubes, the care for which is discussed in Chapter 40. In addition, the patient should be assessed for distention caused by overfilling of the bladder because of an inability to void or a malfunction of the catheters. One of the many benefits of laparoscopic surgery is reduced morbidity to the patient during their postoperative course. Nasogastric tubes are rarely required with minimally invasive surgeries.
Bladder ultrasound scan is a noninvasive method to assess bladder volume for determining bladder distention or postvoid residual urine. This portable battery-operated device can be used at the bedside as a noninvasive replacement of intermittent catheterization (Fig. 41.2). This painless procedure eliminates discomfort, embarrassment, and risks associated with catheterization. Data from the bladder ultrasound scan can be printed and become part of the patient’s chart. Depending on the volume and whether the patient is capable of voiding, straight catheterization should be performed to relieve urinary retention; this procedure is typically done with volumes greater that 200 mL. A bladder ultrasound scan can be repeated as necessary and has been shown to decrease the risk of urinary tract infections associated with intermittent catheterization. The physician’s orders should reflect when they should be contacted with regard to residual urine and recatheterization. The physician will determine whether the patient needs to be discharged with a catheter in place. The perianesthesia nurse should include how to care for the catheter and when to return to see the urologist in any discharge instructions.
FIG. 41.2 Using a bladder scanner to determine amount of urine in the bladder. (From deWit SC, O’Neill P: Fundamental concepts and skills for nursing, ed 4, St. Louis, MO, 2014, Elsevier.)
Management of Discomfort and Pain
Discomfort after genitourinary surgery can be relieved with the administration of various types of opioids as well as other medications. These medications may include intravenous (IV) morphine, hydromorphone, or fentanyl and/or oral oxycodone or hydrocodone or opium suppositories. Pain management may include a pain pump such as IV hydromorphone for inpatients. IV nonsteroidal antiinflammatory drugs (NSAIDs) and/or IV acetaminophen may also be given as a nonopioid adjunct. Patients are gradually converted from IV medication to oral pain medications as soon as possible and before discharge. Many larger hospitals have a pain management service, and surgeons can order pain management services to evaluate the patient for pain when pain is not adequately controlled. In addition, it is important to explain to the patient that these pain medications may cause extreme sedation, nausea, and/or constipation. In an outpatient setting, oral medications such as oxycodone and hydrocodone may be ordered. It is important to stress to patients that they use nonprescription medications for pain such as NSAIDs, as long as there is no sensitivity to them, to decrease the amount of opioids needed. See Chapter 31 for more information on pain management. The physiology of the need to void should be explained to the patient before surgery. The patient should be instructed not to attempt to void around the catheter because exertion of pressure causes the bladder muscles to contract and results in painful bladder spasms. The avoidance of straining around the catheter and of intake of excessive fluids decreases bladder irritability and spasms. As the nerve endings become fatigued, the frequency and severity of the spasms diminish.
Nursing Care After Specific Procedures
Renal and Ureteral Surgery
Procedures that involve the kidneys and ureters include excision of tumors and obstructions to urine flow (e.g., stones), reconstruction of urine outflow tracts, repair of lacerations or injury, correction of deformities, excision of a kidney, and total organ transplant.
General anesthesia is commonly used for surgery on the kidneys and ureters. Depending on the diagnosis, many of these procedures may be done laparoscopically with or without the assistance of the robot (three or four incisions at 5 to 12 mm each are used and as many as seven 5-to 12-mm incisions when using the robot). The incisions for a laparoscopic approach will depend on the anatomy and the position the surgeon is most comfortable suturing laparoscopically (robotic assistance makes suturing much easier if the surgeon does not feel comfortable suturing laparoscopically).15–18 The kidneys are usually approached posteriorly through an incision that requires resection of the eleventh or twelfth rib. The surgical approach to the ureters is made through muscle-splitting flank incisions (Fig. 41.3).1,2 The perianesthesia course for these patients is usually smooth and involves general care and maintenance of urinary tract function. The patient should be placed in a position that avoids tension on suture lines or as indicated by the surgeon.
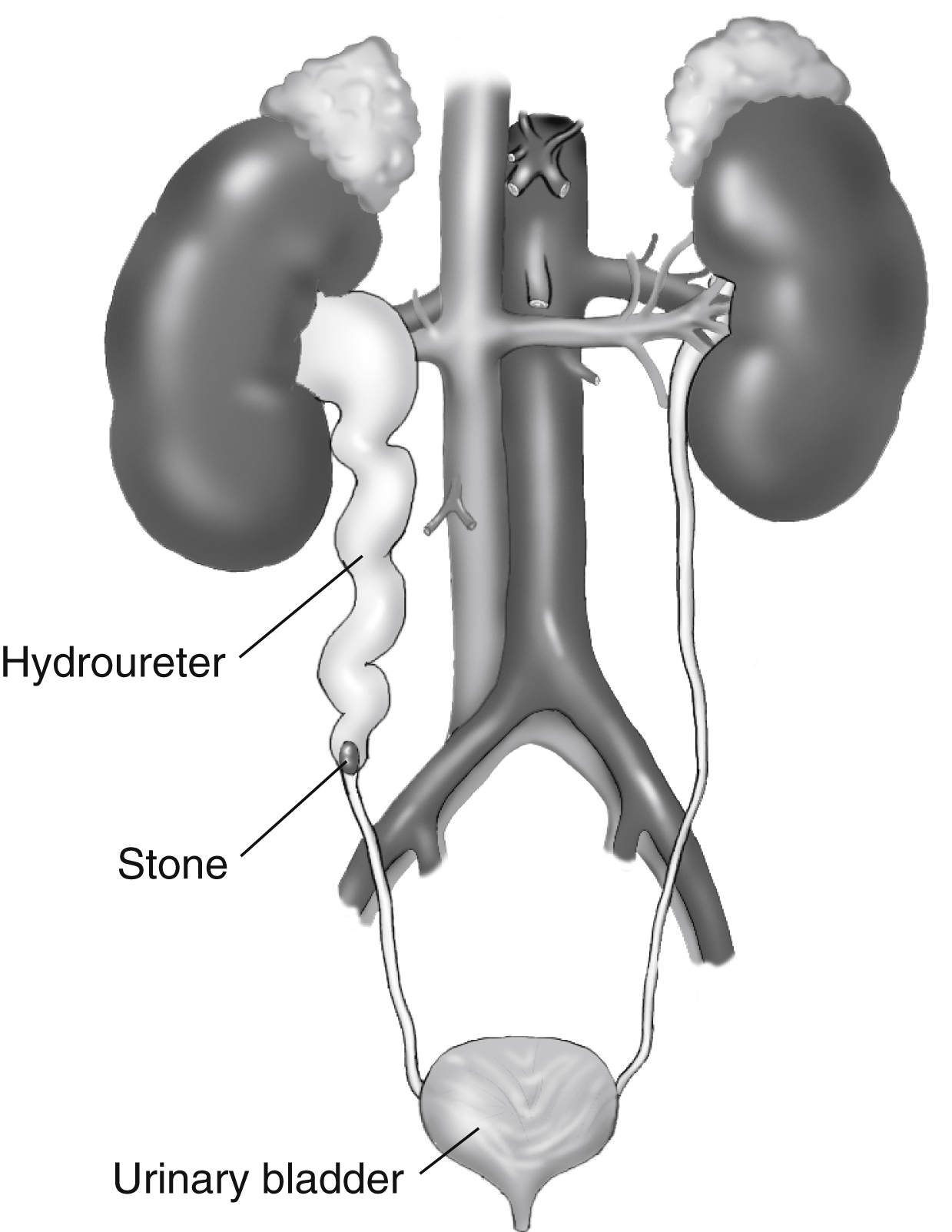
FIG. 41.3 Hydroureter is caused by obstruction in the lower part of the ureter. (From Leonard PC: Building a medical vocabulary, ed 9, St. Louis, MO, 2015, Elsevier.)
All surgical patients are at risk for fluid volume deficit from the intake restrictions before surgery and from the decreased intake after surgery, possibly related to postoperative nausea or vomiting. Maintenance of exceptionally accurate intake and output records is important. Low urine output should be reported to the surgeon.
Dressings should remain dry and intact unless drains are used in which case dressings should be weighed when they are removed to determine output via this route. With the determination of output from the dressings, the dressings should be weighed before application and again at removal and the difference subtracted (1 g equals 1 mL of output). Patients with drains or stomas may need a small plastic bag over the area to collect drainage that consists primarily of urine. Drainage bags should be emptied frequently. If the bags are allowed to fill to capacity, the continual flow of urine is interrupted.
Skin care for these patients is important. Urine should not be allowed to remain on the skin. Plain water should be used to cleanse the skin, which should be carefully dried. No powders, lotions, or harsh skin preparations should be applied to the skin. If a ureteroileostomy has been performed, the stoma must be inspected frequently to ensure adequate vascularization. If the skin turns a bluish hue, the surgeon should be notified immediately.2,9
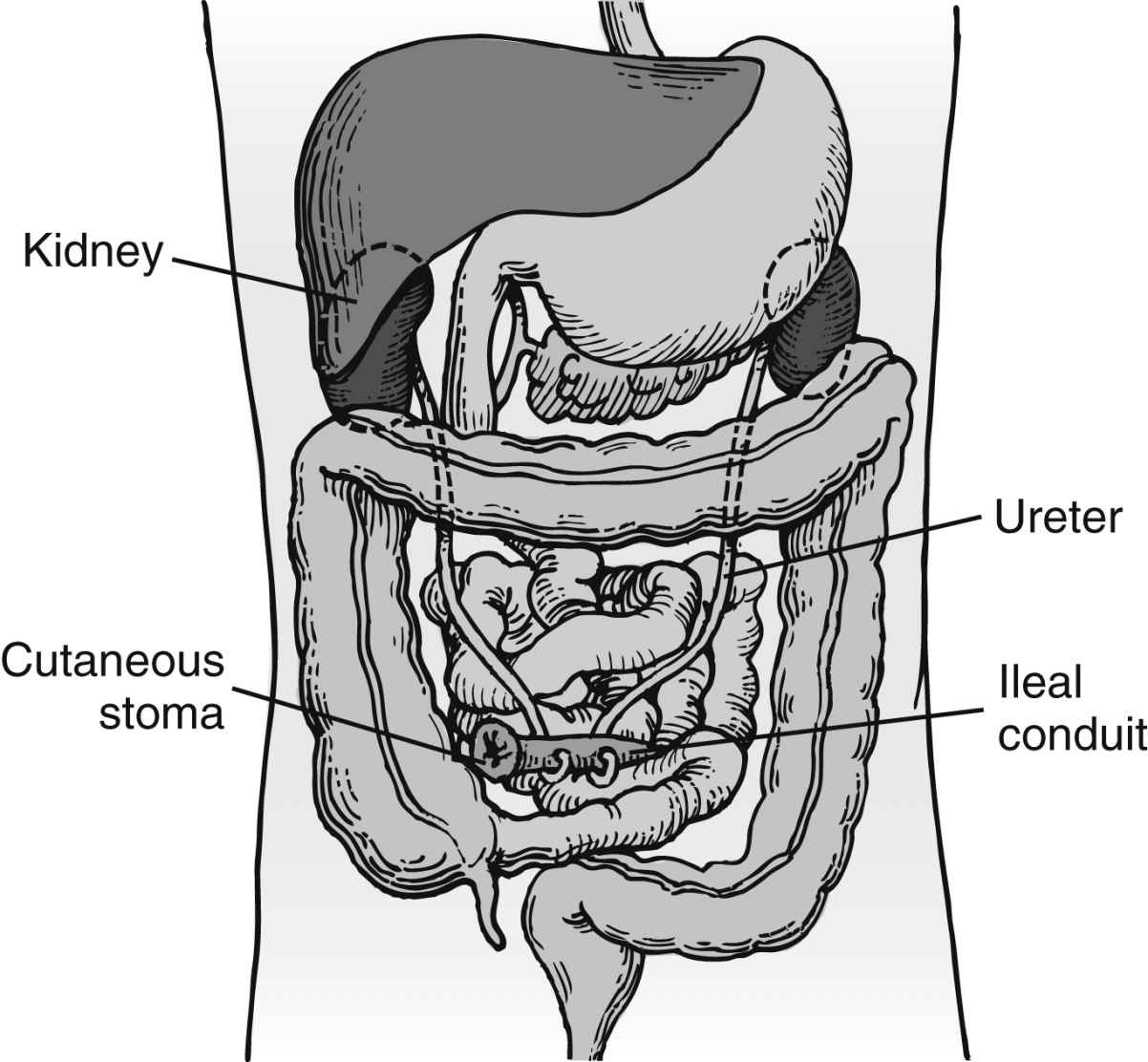
A urinary catheter is often in place and receives care as previously discussed. Fluid intake is increased both orally and parenterally to keep blood clots from forming in the ureters or bladder. Intestinal decompression may be necessary and is accomplished via nasogastric tube (see Chapter 40). Decompression is essential when an ileal conduit procedure (ureterostomy) is performed to allow healing of the intestinal anastomosis (Fig. 41.4).2 Any evidence of abdominal distention should be reported to the surgeon immediately.
Extracorporeal Shock Wave Lithotripsy
After extracorporeal shock wave lithotripsy, the patient may be admitted to the PACU for a brief period of observation. Vital signs should be monitored as with any renal or ureteral surgery. Fluids should be increased, and intake and output monitored carefully. Initially, the color of the urine may be cherry red to pink because of trauma from surgery; this condition may take several hours to clear. Petechiae, redness, and bruising may be seen on the skin at the site of lithotripsy. These petechiae should be documented by the perianesthesia nurse on assessment in the PACU. The patient may have pain from the force of the shock waves. This pain is usually localized to the skin and may be relieved with ice packs. Renal colic pain may also be experienced as the fragments of pulverized stones pass through the lower urinary tract.2,9
Ureteroscopy
Since the 1980s, rigid ureteroscopy has been used for the removal of distal ureteral calculi.1 Today, flexible and rigid ureteroscopy is used for the diagnosis and treatment of stones, fulguration of epithelial tumors, analysis of gross hematuria, and management of ureteral strictures.1,2 Complications are rare but include perforation of the ureter; therefore, close observation of color and amount of urine output should be maintained. All urine should be strained, and any calculous fragments should be collected for inspection and identification. Ureteral stents are commonly placed during this procedure to facilitate urine flow and prevent obstruction or ureteral colic caused by edema. If the surgeon has elected to externalize the stent suture, patients should be educated on its care.
Percutaneous Nephrolithotomy
Large stones that are not easily removed with ureteroscopy can be removed through a percutaneous tract into the renal collecting system. Local anesthesia or moderate sedation is used to establish the percutaneous nephrostomy tract with the guidance of fluoroscopy or ultrasound scan. A plastic sheath is left in place through which a rigid or flexible nephroscope can pass. Stones smaller than 1 cm can be removed manually with a grasping forceps. General anesthesia is used for the surgical procedure itself. For larger stones lithotripsy is used according to the surgeon’s preferred method and the location of the stone.2
FIG. 41.4 Ileal conduit created from isolated segment of ileum with ureters anastomosed to segment between closed end and external stoma. Urinary collection device must be placed over incontinent stoma. Incontinent urinary diversion carries urine from kidneys through implanted ureters and ileal conduit to stoma. (From Phillips N: Berry and Kohn’s operating room technique, ed 13, St. Louis, MO, 2017, Elsevier.)
Postoperative nursing care should include the consideration of surgical complications and all postanesthesia considerations. Blood loss from damage to an intrarenal artery is the most significant complication of percutaneous nephrolithotomy. Extravasation of the irrigation solution used during surgery is another complication. Rare complications include damage to the surrounding organs caused by perforation with the placement of the percutaneous nephrostomy tube. The nephrostomy tube may be left in place for 1 to 5 days. Pain at the nephrostomy site may require management with opioids. As with all genitourinary surgeries, adequate fluid intake is encouraged.2,10
With each of the types of renal stone removal procedures, nursing care should include patient education on types of stones, diet for the prevention of stones, and fluid intake to improve the excretion of stones and prevention of new stone formation. There are five types of renal stones: calcium oxalate, calcium phosphate, uric acid, struvite, and cysteine.2 Of these, the calcium oxalate stone is the most common. Each stone has different diet and fluid intake recommendations and restrictions. Patients should be educated on the importance of follow-up with the surgeon to identify the type of renal stone they are producing. By knowing the chemical makeup of the stone, the surgeon is able to make specific diet recommendations to the patient (Box 41.1).
From Attalla K, Shubha DE, et al.: Oxalate content of food: a tangled web. Urology 84(3):555–560, 2014.
Kidney Transplantation
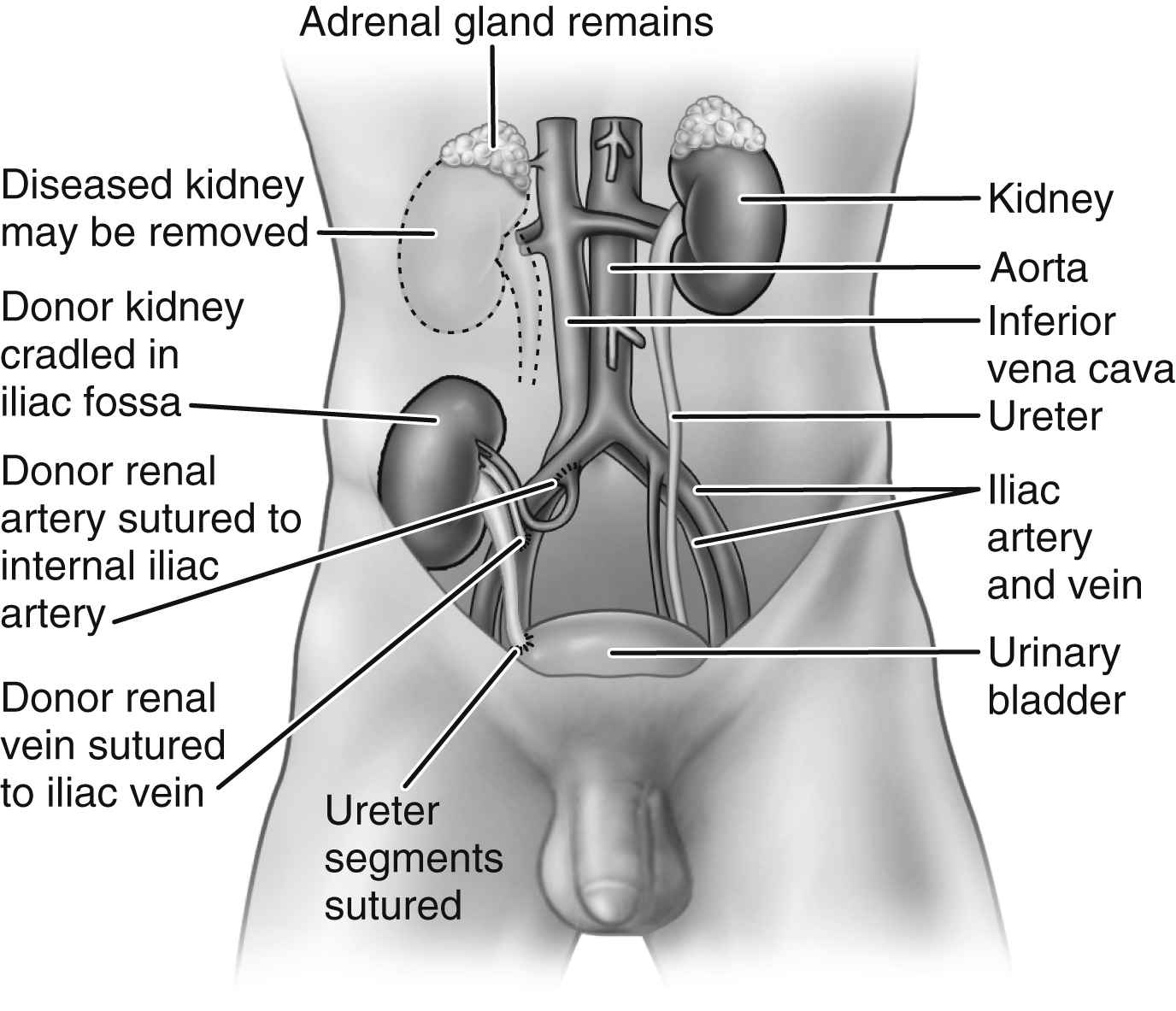
The kidney is a commonly transplanted organ and can be preserved in a viable state for some time (Fig. 41.5). The kidney is relatively easy to remove and implant. Most people have two functioning kidneys and need only one to sustain life (without having to go on dialysis); therefore, kidney transplantation is done only for patients who need the organ to replace a diseased or nonfunctioning solitary kidney. Transplantation can be accomplished two, three, or more times in the same patient with the use of hemodialysis when a functioning kidney is not in place.2
Kidney grafts come from two sources: cadaver donors and living donors. Most living donors are a close blood relative of the recipient. Ideally, an identical twin is the best donor. The closer the recipient and donor are in their blood line, the better the chances for survival of the kidney graft. Although a living related donor is best, cadaver donors are the most common source for kidney graft.2
General anesthesia is the preferred method of anesthesia for both the donor and the recipient in renal transplantation.2 After surgery, care of the living donor is essentially the same as that for the patient who has undergone nephrectomy. All care considered previously for the urologic patient applies as does care for the patient after abdominal incision. If the laparoscopic approach (with or without the use of the robot) is used for the living donor, three to seven stab wounds are found from the trocars (closer to seven for robotic assistance).15–18 Postoperative priorities include accurate intake and output, fluid volume and electrolyte replacement, adequate pulmonary perfusion, and pain and comfort measures.
FIG. 41.5 Transplanted kidney in place. (From Black JM, Hokanson Hawks J: Medical-surgical nursing: clinical management for positive outcomes, ed 8, St. Louis, MO, 2009, Elsevier.)
Only gold members can continue reading. Log In or Register to continue