Anesthesia for cardiac surgery varies by hospital and can also vary by the type of cardiac repair. Ideally, anesthetic management includes drugs that have rapid onset and termination, minimize ischemia, and are nontoxic to myocardial and other tissue.2,3 For example, volatile anesthetics, intravenous vasodilators, and certain intravenous anesthetics have effects on pulmonary vascular resistance. Hemodynamic effects of some anesthetic drugs are shown in Table 35.2.
Procedures
Monitoring
Monitoring (Table 35.3) of the patient’s electrocardiogram (ECG) and direct blood pressure (commonly via the radial artery in the nondominant wrist) is initiated when the patient arrives in the preoperative area. Central lines are usually inserted after transport into the operating room (OR) but occasionally are inserted in another designated location such as the preoperative area. Whether the patient first undergoes intubation before insertion of central lines (i.e., central venous pressure, pulmonary artery catheter) or after line insertion is at the discretion of the anesthesia provider; the sequence varies among institutions. Increasingly, an anesthesia provider inserts a transesophageal echocardiography (TEE) probe routinely to illustrate cardiac function in patients undergoing valve surgery and patients with compromised LV function.3
Incisions
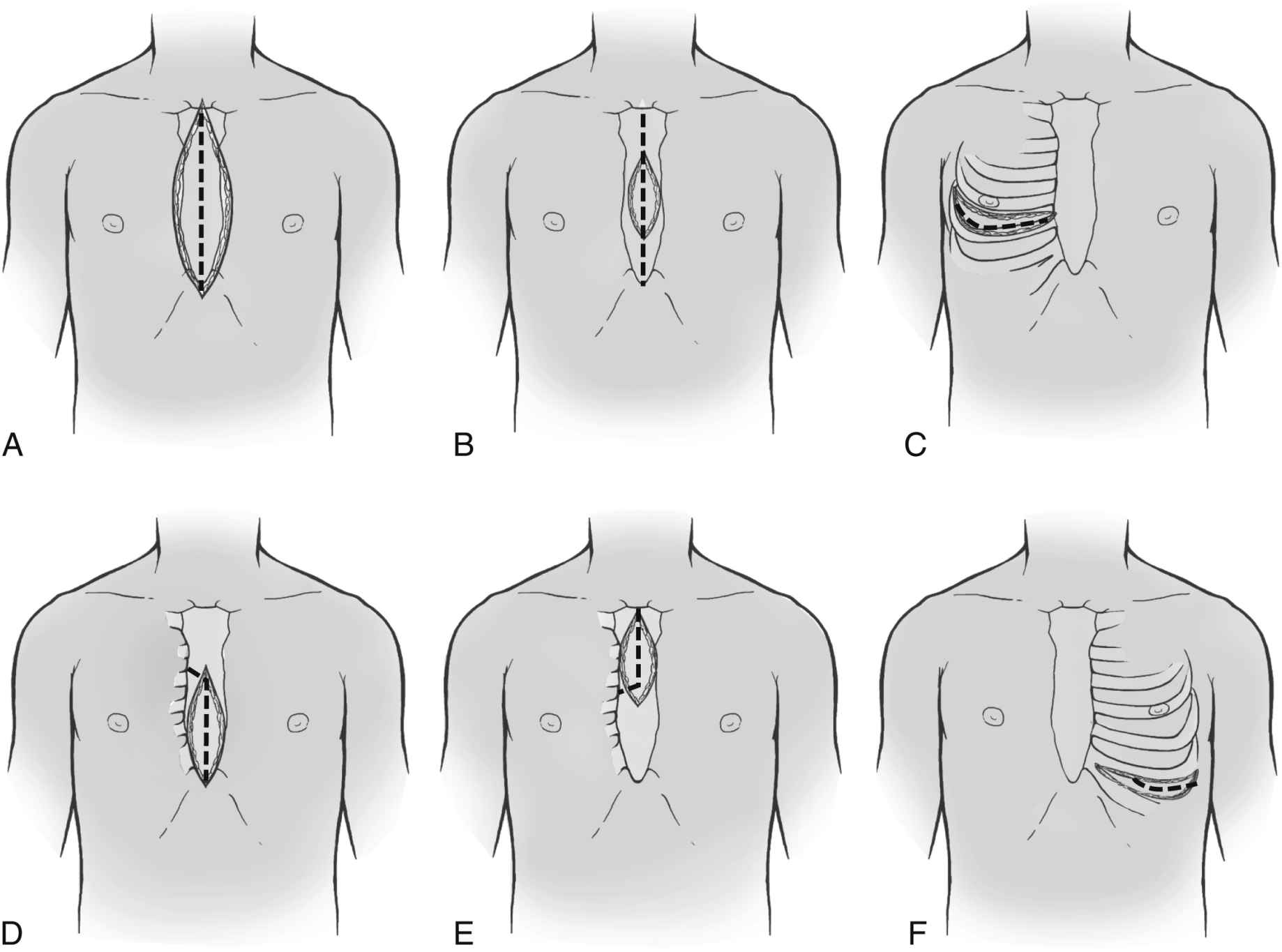
After the patient has been anesthetized, positioned, and washed (prepped), the chest is opened. The most commonly used chest incision in cardiac surgery is the median sternotomy; this is the preferred incision when a thorough assessment of, and complete access to, the heart (as with multivessel coronary artery disease [CAD]) is needed. However, ministernotomy, right or left anterolateral or posterolateral thoracotomy incisions, or transverse sternotomy also may be used (Fig. 35.1). The surgeon splits the sternum with a saw from the sternal notch to the xiphoid process. After the sternum is opened, the exposed pericardial sac is incised anteriorly, and the pericardial edges are tacked up along the chest wall incision to allow complete access to the entire pericardium without the necessity of entering the pleural cavities. Minimally invasive surgery uses smaller incisions and can speed patient recovery, enable the patient to return faster to normal activities, and reduce costs.
Table 35.2
Hemodynamic Effects of Anesthetic Drugs
Table 35.3
Physiologic Monitoring
FIG. 35.1 Traditional and less invasive thoracic incisions (dotted lines represent chest wall incisions). A, Traditional sternotomy. B, Full sternotomy with limited skin incision. C, Right thoracotomy can be used for mitral valve procedures. D, and E, Partial lower and upper sternotomy incisions used mainly for valve procedures. F, Left anterior thoracotomy can be used for single coronary bypass graft to left anterior descending coronary artery. (From Braunwald E, et al., editors: Heart disease, ed 6, Philadelphia, PA, 2001, Elsevier.)
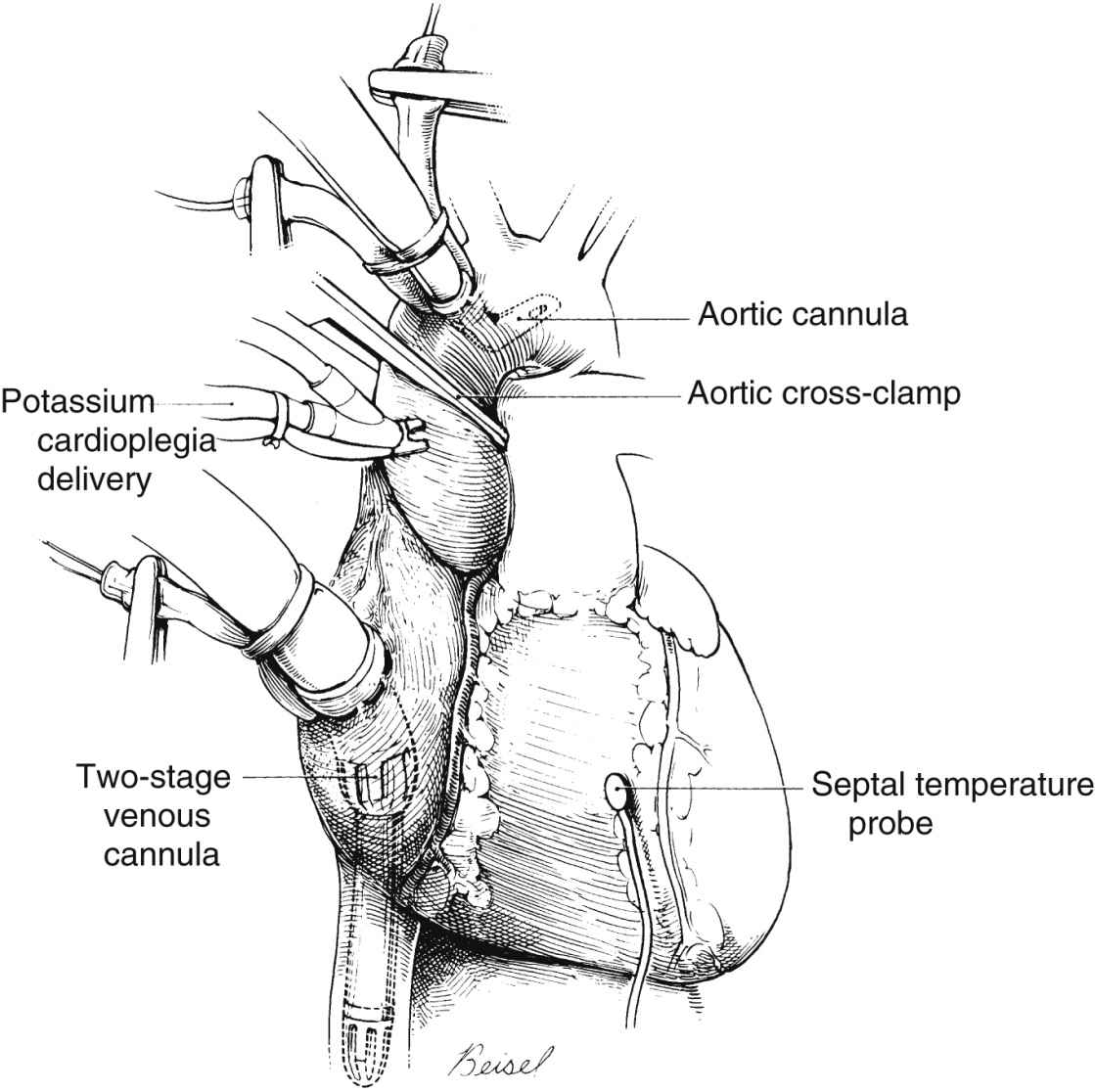
FIG. 35.2 Antegrade cardioplegia infusion catheter is inserted proximal to aortic cross clamp and arterial infusion cannula. Two-stage (single) venous cannula drains systemic venous return. Openings in distal end of cannula drain blood from lower body; openings in midportion of cannula (within right atrium) drain blood returning from upper body and coronary venous drainage exiting from coronary sinus. Septal temperature probe monitors myocardial septal temperature. (From Waldhausen JA, et al.: Surgery of the chest, ed 6, St. Louis, MO, 1996, Elsevier.)
Cardiopulmonary Bypass
Systemic venous return to the heart flows by gravity drainage (the level of the patient needs to be above that of the bypass machine to facilitate drainage) into one or two large-bore (e.g., 32F to 36F) cannulas inserted into the right atrium (RA). The addition of vacuum assistance (i.e., suction) to facilitate venous drainage allows insertion of smaller cannulas.
With the single two-stage cannula (Fig. 35.2), openings in the distal tip drain blood returning from the inferior vena cava (IVC), and openings in the middle portion of the cannula drain venous blood from the superior vena cava (SVC) and the coronary circulation exiting from the coronary sinus. Some blood enters the RA and the pulmonary circulation. With double cannulation (Fig. 35.3), individual cannulas are inserted into the IVC and the SVC, thereby forcing all venous return into the cannulas. Generally, the two-stage cannula is used for coronary artery bypass grafting (CABG) and aortic valve surgery when total right side decompression is not generally needed and blood entering the right side of the heart does not obscure the surgical field. Individual (double) venous cannulation can be used for procedures in the right side (e.g., tricuspid valve repair) to keep the right heart free of blood. Occasionally, two cannulas can be used when greater decompression of the RA is necessary (e.g., mitral valve surgery).
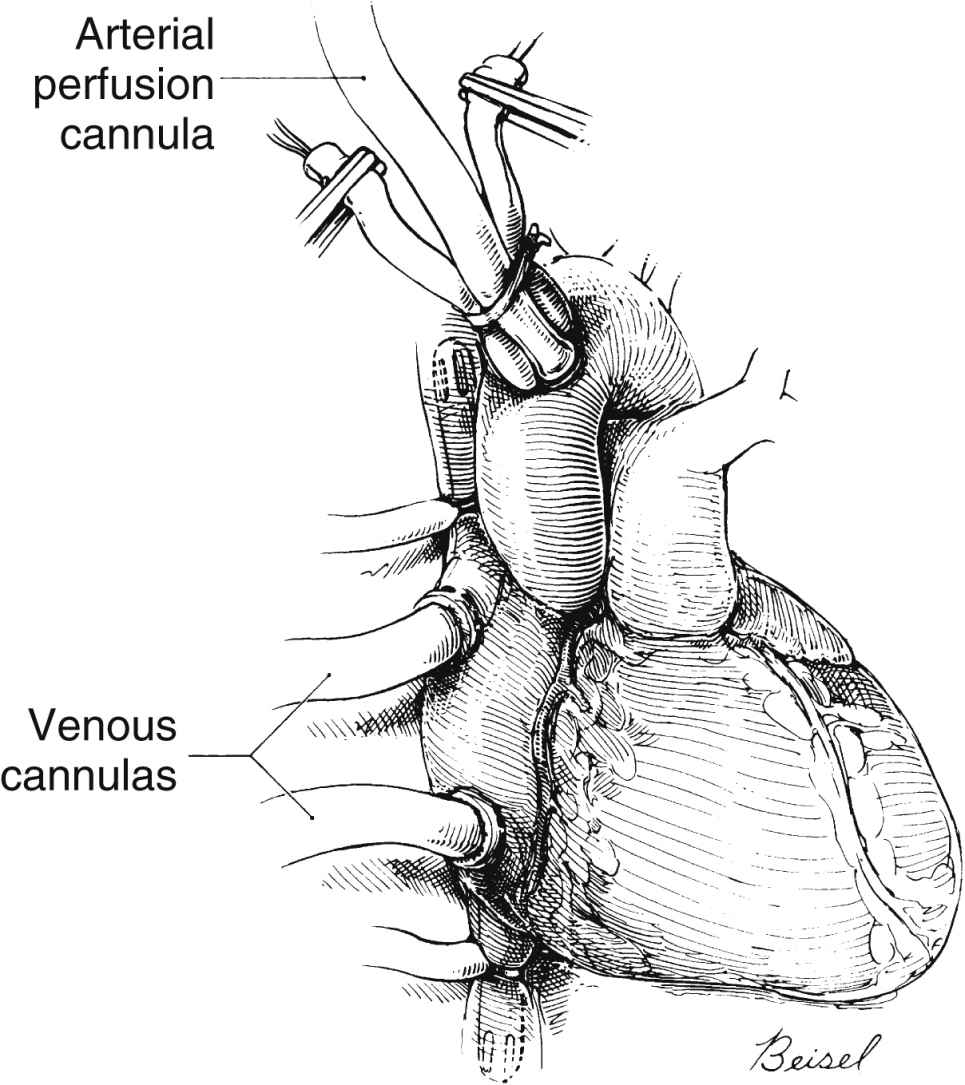
FIG. 35.3 Double venous cannulation. One cannula is inserted into inferior vena cava and the other into superior vena cava. Also shown is arterial infusion catheter. (From Waldhausen JA, et al.: Surgery of the chest, ed 6, St. Louis, MO, 1996, Elsevier.)
After the blood is oxygenated, it is pumped into the systemic circulation via an arterial cannula, commonly located in the aorta (see Fig. 35.3). When aortic pathology (e.g., aortic aneurysm) makes aortic cannulation risky, the femoral artery can be cannulated (retrograde flow) for arterial return. The axillary artery may be needed when the aorta or both of the femoral arteries are unavailable.
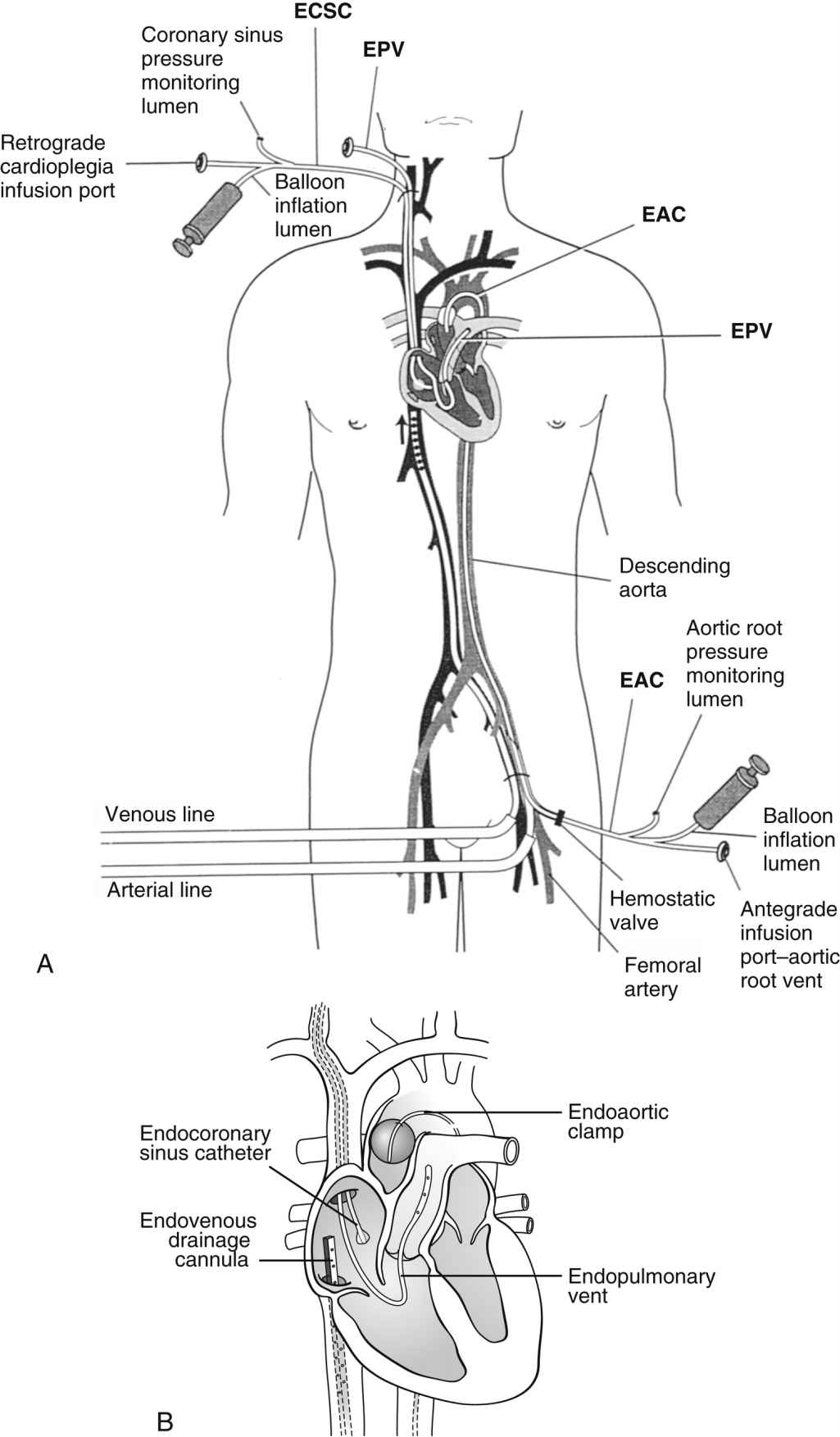
In addition to the standard cannulation techniques for cardiopulmonary bypass (CPB), minimally invasive systems use endovascular catheters (Fig. 35.4). A venous catheter is inserted into the femoral vein, and the arterial cannula is placed into the femoral artery. The ipsilateral femoral artery is also used for insertion of a multilumen catheter. One lumen serves as an endovascular cross clamp that occludes the aorta with inflation of an intraaortic balloon at the tip of the catheter, and the other lumen can be used for infusion of antegrade cardioplegia. Pressure lines, venting catheters, and a coronary sinus retrograde cardioplegia catheter can be inserted via the jugular vein. This system does not require median sternotomy and is an important adjunct for minimally invasive surgery.4
FIG. 35.4 Minimally invasive cardiopulmonary bypass technique. A, Positioning of endovascular catheters. B, Correct positions of endocoronary sinus catheter, endoaortic clamp, endovenous drainage cannula, and endopulmonary vent for port-access cardiopulmonary bypass. EAC, Endoaortic clamp; ECSC, endocoronary sinus catheter; EPV, cardiopulmonary vent. (A, From Toomasian M, et al.: Extracorporeal circulation for port-access cardiac surgery. Perfusion 12:83, 1997. B, From Kaplan J, editor: Kaplan’s cardiac anesthesia, ed 5, Philadelphia, PA, 2006, Elsevier.)
BOX 35.1Checklist for Initiation of Pump
• Heparin administered
• Activated coagulation time checked and at least 350 to 400 seconds
• Muscle relaxant adequate (or infusion turned on for maintenance)
• Inotropic infusions turned off
• Pupil symmetry assessed for later comparison (unilateral dilation may indicate unilateral carotid perfusion on cardiopulmonary bypass)
• Pulmonary artery catheter (if used) pulled back 5 cm
• Urinary output emptied before bypass (start anew with initiation of bypass)
• Proper functioning of all monitors ensured
From Lemmer JH, Vlahakes GJ: Handbook of patient care in cardiac surgery, ed 7, Philadelphia, PA, 2010, Lippincott Williams & Wilkins; Bojar RM: Manual of perioperative care in adult cardiac surgery, ed 5, Oxford, UK, 2011, Wiley-Blackwell.
BOX 35.2Checklist for Weaning from the Pump
• Patient is warm (to at least 36° C)
• Heart rhythm has returned
• All monitors are functioning; electrocardiogram, pulmonary artery tracing, arterial line tracing, central venous pressure reflect heart filling
• Heart rate is 70 to 100 beats/min (<60 beats/min is reduced cardiac output; ≥120 beats/min is detrimental to left ventricular filling)
• Infusions are prepared as necessary
• Lungs are inflated but kept out of the surgeon’s field
• Pressure becomes pulsatile as ventricles fill
• Blood is drawn for measurement of electrolytes, hematocrit, arterial blood gases, and activated clotting time
• The surgeon clamps the venous drainage cannula and removes the cannula
• Patient is off pump
From Lemmer JH, Vlahakes GJ: Handbook of patient care in cardiac surgery, ed 7, Philadelphia, PA, 2010, Lippincott Williams & Wilkins; Bojar RM: Manual of perioperative care in adult cardiac surgery, ed 5, Oxford, UK, 2011, Wiley-Blackwell.
A number of risks are associated with the use of CPB (e.g., particulate or air embolus), and some form of checklist is often used before CPB is instituted (Box 35.1) and before the patient is weaned from CPB (Box 35.2). Such checklists help to enhance the safety of CPB. In addition, the clinical sequelae of CPB can affect all body systems.4 Caregivers in the postoperative period should be aware of the possible effects of CPB (Table 35.4).
CPB is not always required. So-called off-pump procedures for myocardial revascularization can be performed while the heart is beating with the use of special devices to isolate the section of the coronary artery to be grafted; patients with a heavily calcified aorta are candidates so that the surgeon can avoid clamping a calcified aorta and risking dislodging a calcium particle, which can embolize to the brain. For procedures that require entry into the chambers of the heart (e.g., valve replacement), CPB and myocardial protection are necessary for perfusion of the body, avoidance of air emboli that originate from the open cardiac chamber, and myocardial preservation.
Myocardial Protection
The goal of myocardial protection is to conserve cardiac energy resources; the goal is achieved with induced hypothermia and rapid diastolic arrest. Hypothermia reduces the metabolic rate (and therefore the energy demands) of the tissue being cooled, thereby conserving the heart’s energy resources for the resumption of work once the heart starts to beat again.
For most cardiac procedures of less than 1 hour of induced cardiac arrest (e.g., CABG), the perfusionist cools the systemic circulation from a normal temperature of 37° C (98.6° F) to approximately 34° C (93.2° F). The cardioplegia solution is cooled to a lower temperature for intracardiac cooling as a method of myocardial protection. For procedures with a longer cross-clamp time, the systemic temperature may be further reduced to protect the brain, kidneys, and other organs while the heart is arrested by reducing energy demands and limiting ischemic injury. Topical cooling of the heart with cold lavage or frozen “slush” placed on the heart and in the pericardial well helps to achieve transmural cooling.
Although induced hypothermia plays an important role in minimization of tissue ischemia during selected portions of cardiac procedures, inadvertent hypothermia has become an important consideration for cardiac patients because of associated risks for perioperative complications. Before surgery, shivering increases myocardial oxygen demands and further taxes hearts that have diminished myocardial energy supplies. During surgery, before and after CPB, inadvertent cooling of the patient is associated with increased surgical bleeding and a diminished immune response. After surgery, hypothermia contributes to patient discomfort, impaired wound healing, prolonged bleeding, longer lengths of stay, and cardiac events such as ischemia and tachyarrhythmias.3 Active measures — such as the application of forced warm air devices before surgery, during the intraoperative period (before and after induced hypothermia), and the postoperative period—may be employed. Additional measures include the use of intravenous fluid warmers, covering the blanket to reduce heat loss, and increasing ambient room temperature to maintain normothermia.
Table 35.4
Effects of Cardiopulmonary Bypass
Adapted from Lighthall GK, Olejniczak M: Routine postoperative care of patients undergoing coronary bypass grafting on cardiopulmonary bypass. Semin Cardiothorac Vasc Anesth 19(2):78–86, 2015; Rhee C, Sax PE: Evaluation of fever and infections in cardiac surgery patients. Semin Cardiothorac Vasc Anesth 19(2):143–153, 2015; Bainbridge D, Cheng DC: Early extubation and fast-track management of off-pump cardiac patients in the intensive care unit. Semin Cardiothorac Vasc Anesth 19(2):163–168, 2015; Lemmer JH, Vlahakes GJ: Handbook of patient care in cardiac surgery, ed 7, Philadelphia, PA, 2010, Lippincott Williams & Wilkins; Bojar RM: Manual of perioperative care in adult cardiac surgery, ed 5, Oxford, UK, 2011, Wiley-Blackwell.
Rapid diastolic arrest conserves existing cellular energy resources (e.g., adenosine triphosphate/ATP) by avoiding the energy-expensive state of ventricular fibrillation before the heart achieves an arrested state. Quick arrest of a beating heart (e.g., 10 to 20 seconds) enhances myocardial energy conservation. Potassium is the most commonly used arresting agent, but the solutions may also contain electrolytes, buffers to maintain appropriate pH, glucose, metabolic substrates, calcium antagonists, tromethamine, heparin, and antiarrhythmic agents. The carrying solution can be crystalloid or blood (preferable for its oxygen-carrying capacity).3
Methods of infusing cardioplegia include the antegrade and retrograde routes and the direct coronary ostial route of infusion. With the antegrade method, a needle catheter is inserted into the anterior aorta proximal to the aortic cross clamp (see Fig. 35.2). The cardioplegia solution is infused with sufficient pressure to close the aortic valve. With the cross clamp applied distally and a competent aortic valve proximally, the only paths for the solution to travel are the right and left coronary ostia lying between the cross-clamped aorta and the closed aortic valve. In patients with aortic valve insufficiency, cardioplegia flow into the coronary ostia is significantly reduced because the incompetent aortic valve provides a lower pressure pathway into the inner ventricular chamber, thereby distending the heart and increasing myocardial wall tension. Retrograde delivery is indicated in the presence of coronary artery lesions that impair the transmural distribution of the cardioplegia when delivered solely by the antegrade route. For the retrograde route, the surgeon inserts a catheter through a stab wound into the right atrial wall and threads the catheter into the coronary sinus. The cardioplegic solution infused into the coronary sinus flows retrograde through the cardiac veins and arteries. The solution exits via the coronary ostia, where it is removed by suction.
In addition to thermal and pharmacologic interventions, other strategies to achieve adequate myocardial energy conservation include implementing actions that consistently maximize myocardial energy supplies and minimizing myocardial energy demands. Surgeons and assistants use caution in touching the heart before bypass to lessen the risk of ventricular fibrillation. Anesthesia providers pharmacologically decrease cellular oxygen demand and increase cellular oxygen supply. Other considerations in protecting the heart and preventing error include minimization of cross-clamp time with availability of the appropriate supplies and equipment, a plan for surgery (jointly developed by surgeons, anesthesia providers, perfusionists, and nursing personnel), anticipation and ability to respond to potential risks and complications applicable to one’s professional responsibilities and skills, implementation of safety procedures, and frequent and collaborative communication.
Surgery for Coronary Artery Disease
CAD remains the leading cause of death among men and women.5 Left heart cardiac catheterization is commonly performed for identification of areas affected by obstructive atherosclerotic CAD. Selective coronary angiography with an injection of contrast medium into the right and left coronary ostia illustrates coronary anatomy, distal coronary perfusion, the location of atherosclerotic lesions, the status of coronary collateral circulation, and the percentage of narrowing of coronary arteries affected by CAD. Dye is injected into the LV (ventriculography) to determine wall motion (e.g., hypokinesia, dyskinesia, paradoxical motion), and valvular function (e.g., mitral regurgitation [MR], prosthetic valve function). Generally, a right heart catheterization yields data concerning the inferior and superior vena cava, the right atrium and ventricle, tricuspid and pulmonary valves, and the pulmonary vasculature.
Percutaneous coronary interventions, specifically angioplasty with stent insertion, can be performed for discrete coronary lesions. Complications from the interventional procedure include prolonged chest pain, myocardial infarction (MI), coronary spasm, or coronary artery dissection that can necessitate emergency CABG. Evidence supports surgical revascularization (i.e., CABG) over percutaneous coronary interventions in patients with three-vessel and left main CAD.6,7
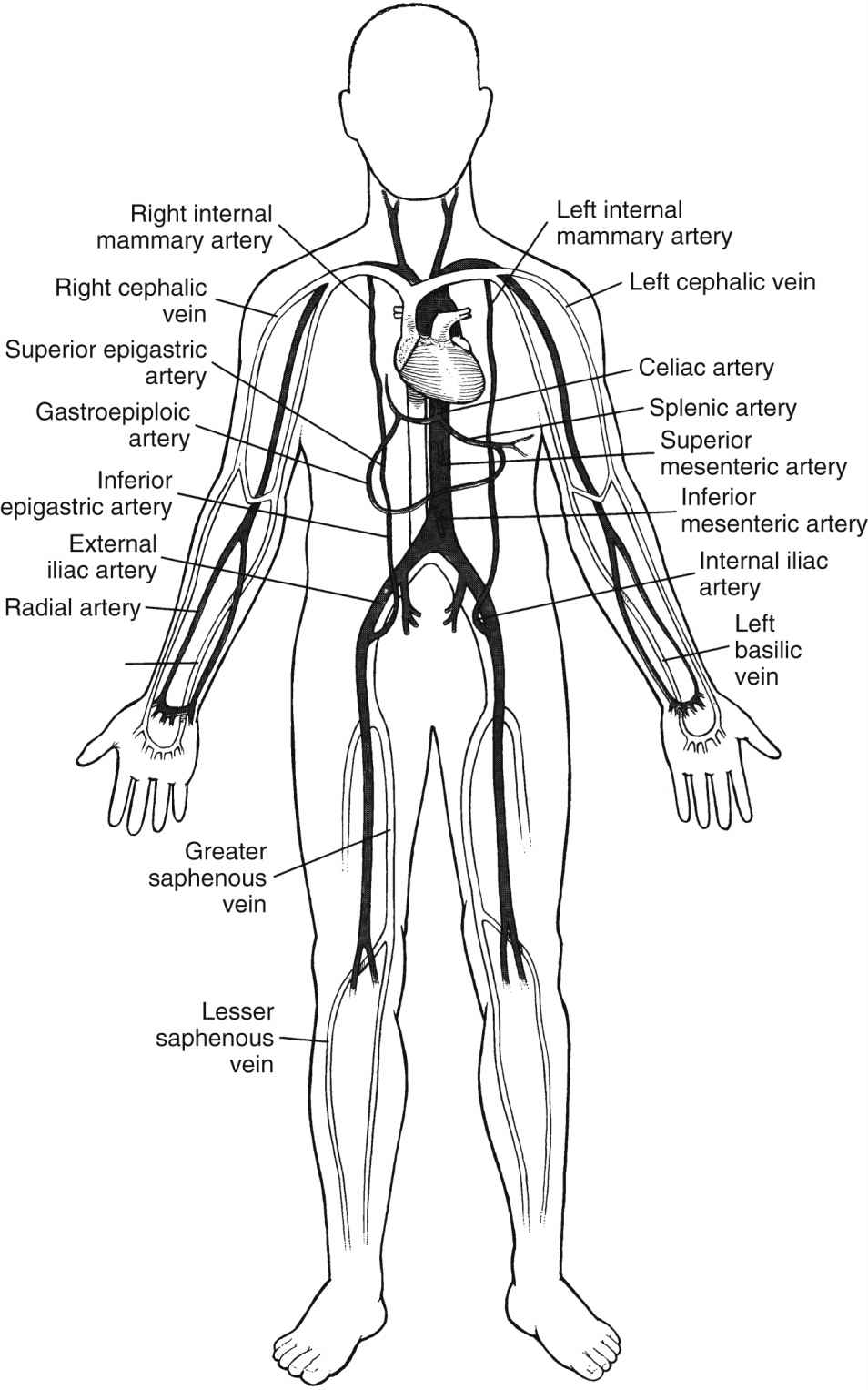
When CABG is recommended for patients, the numbers and types of bypass grafts (e.g., saphenous vein, internal mammary artery [IMA]) are assessed. Fig. 35.5 illustrates possible arterial and venous autologous conduits. Grafts from cadaver human saphenous vein and human and bovine umbilical vein and synthetic grafts have been used when other conduits were unavailable. CAD is a progressive disease, and CABG does not cure CAD; its purpose is to increase blood flow to the myocardium beyond the obstructive lesions. Retardation of the atherosclerotic process requires lifestyle changes and pharmacologic support (e.g., statins). Gender-based differences in CABG outcomes have been reviewed, and guidelines have been published to provide evidence for the selection of techniques.5
FIG. 35.5 Arterial and venous conduits for coronary bypass surgery. (From Seifert PC: Cardiac surgery, St. Louis, MO, 2002, Elsevier.)
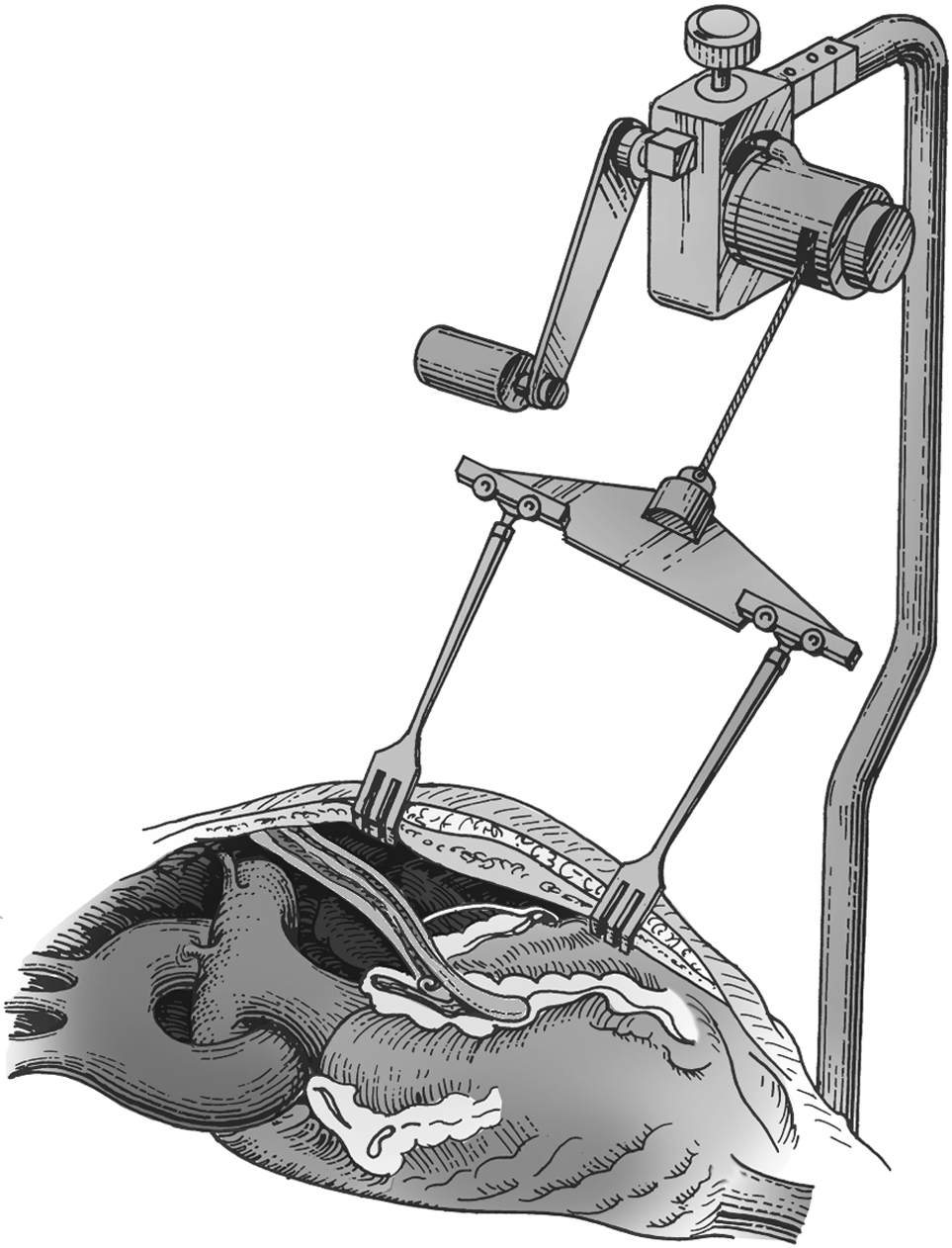
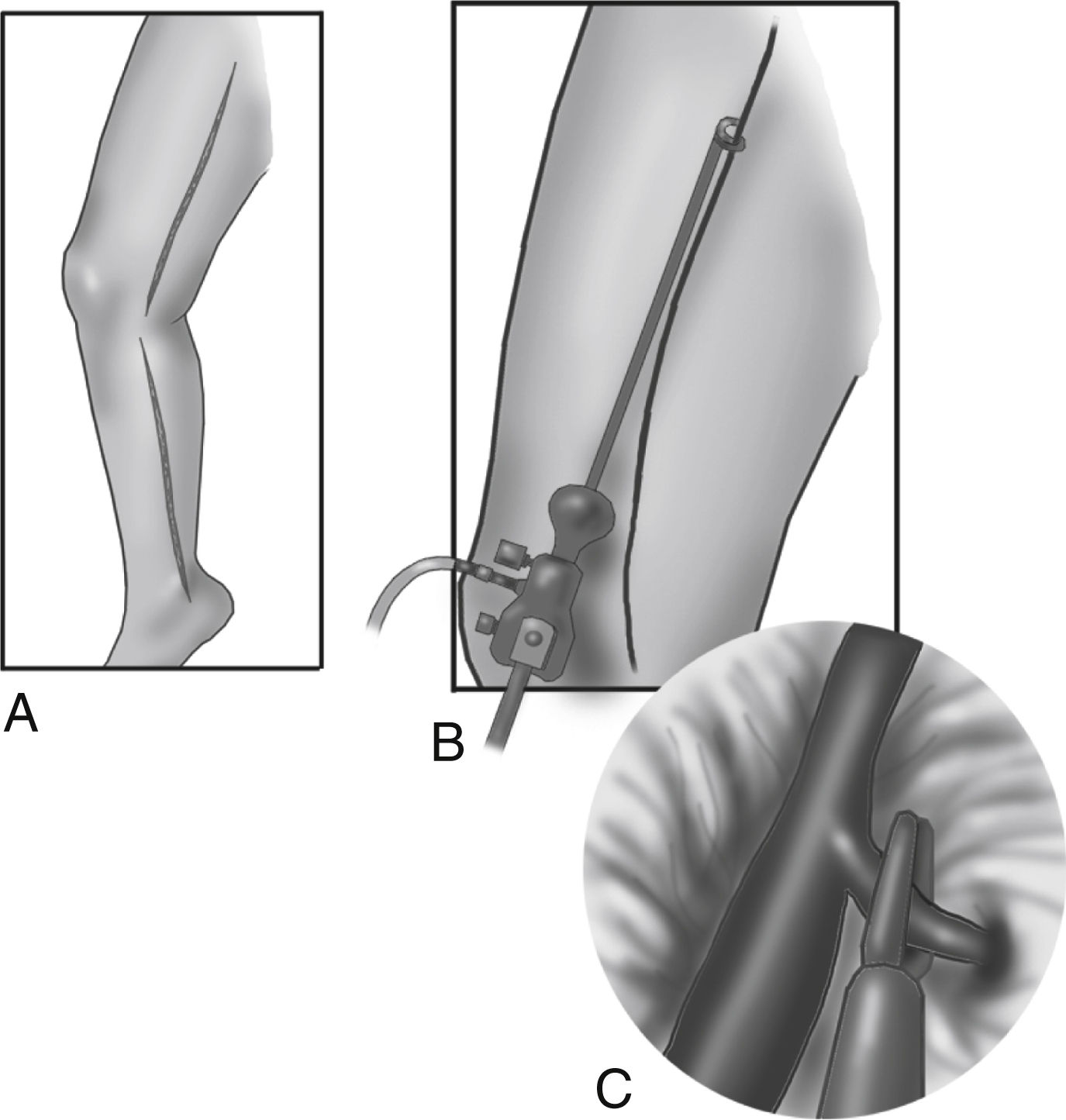
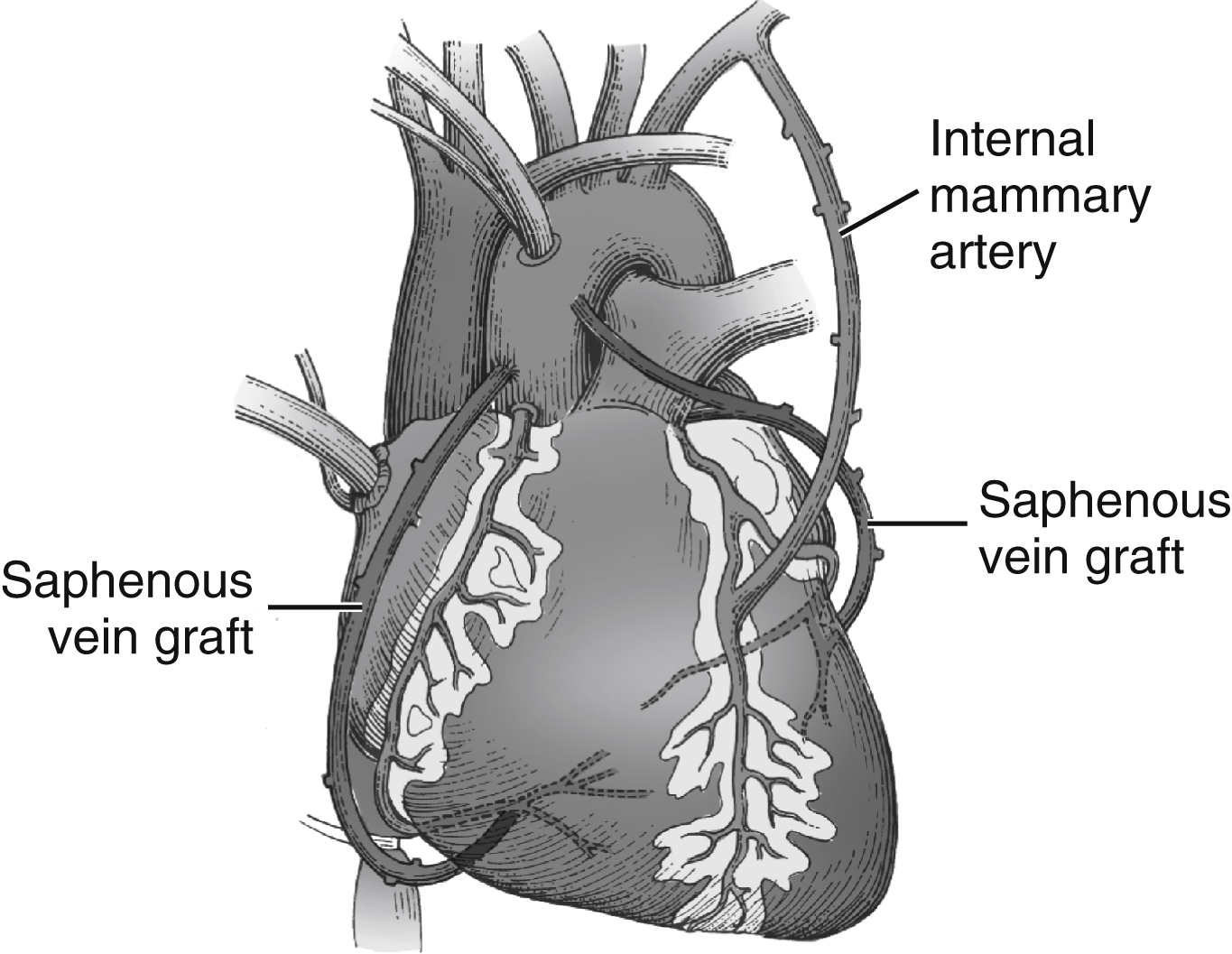
Once the sternum is opened, the surgeon dissects the required length of the IMA (Fig. 35.6). The IMA is dissected from its retrosternal bed to the required length, leaving intact the proximal attachment to the left subclavian artery. The assistant harvests additional bypass conduits such as the saphenous vein (Fig. 35.7) or the radial artery.8 The greater saphenous vein is commonly harvested with video-assisted endoscopic techniques.9 Because leg veins have valves that facilitate flow toward the right heart, reversal of the vein is necessary so that flow as a bypass graft is not impeded. After conduit harvesting is completed or if another procedure is planned (e.g., valve repair), the surgeon proceeds to cannulate for CPB. The body is cooled to the desired temperature, and the heart is arrested with cardioplegia. The surgeon then proceeds to attach the grafts to the heart. The left IMA is commonly used in bypass of the left anterior descending coronary artery. The distal anastomosis is created by attaching the end of the graft conduit to the side of the coronary artery; proximally, the IMA graft remains attached to the subclavian artery. For vein grafts, the surgeon attaches the proximal end of the vein to an opening created in the side of the proximal aorta. Vein grafts may be attached to the diagonal, obtuse marginal, posterior descending, or right coronary arteries. Fig. 35.8 illustrates the IMA graft to the left anterior descending (LAD) coronary artery and saphenous vein grafts to the obtuse marginal (OM) coronary and the posterior descending (PDA) coronary arteries.
FIG. 35.6 Dissection of left internal mammary artery from retrosternal bed with use of special retractor that elevates sternal border. (Courtesy of Rultract, Inc., Cleveland, OH.)
FIG. 35.7 Minimally invasive approach to saphenous vein harvesting. A, Traditional open incision. B, Insertion of endoscopic camera and dissector. C, Venous tributaries cut and clipped, cauterized, or ligated to prevent leaking of blood. (From Zipes DP, et al.: Braunwald’s heart disease: a textbook of cardiovascular medicine, ed 7, Philadelphia, PA, 2005, Elsevier.)
FIG. 35.8 Coronary artery bypass grafts with left internal mammary artery to left anterior descending coronary artery, and saphenous vein grafts to obtuse marginal and posterior descending distal right coronary arteries. (From Braunwald E, et al., editors: Heart disease, ed 6, Philadelphia, PA, 2001, Elsevier.)
Evidence-Based Practice
Surgical teams continue to provide safer care with fewer errors and preventable events. However, errors continue to occur. The causes are related to technical (clinical skill) and nontechnical (communication, situational awareness) factors as well as the frequent introduction of new equipment, devices, and surgical techniques. Sanchez, Ferdinand, and Fann provide an overview of safety science and distinguish between preventable and nonpreventable events.
Implications for Practice
Characteristics of safe organizations
1. Learn from failure
• Examine “near misses” and unsafe situations
• Correct equipment failures, medication errors, and scheduling mistakes
• Examine systemic, technical, and other types of errors
2. Identify the types of mistakes
• Differentiate among Skill, Rule, and Knowledge (SRK) classes of mistakes
• Skill-based mistakes: Slips and lapses
• Rule-based mistakes: Incorrect application of a rule
• Knowledge-based mistakes: Knowledge gap
3. Adapt behaviors of high-reliability organizations
• Anticipate problems and failures
• Do not be too quick to simplify; may make system more vulnerable to failure
• Be sensitive to consequences of change on the entire organization
• Commit to staff resilience
• Assist individuals to recover from unexpected events
• Train for worst-case scenarios
• Defer to individuals with expertise in relevant knowledge and experience—regardless of rank
4. Reflect attributes of safety-focused teams
• Train together
• Encourage team members to voice concerns
• Brief team in anticipation of problems
• Clarify roles of team members
• Provide mechanisms for conflict resolution
• Share accountability
• Learn about new technology (including problem solving)
• Define clearly the boundaries of actions and behaviors
• Engage in open, robust and active communication
Source: Sanchez JA, Ferdinand FD, Fann JI: Patient safety science in cardiothoracic surgery: an overview. Ann Thorac Surg 101:426–433, 2016.
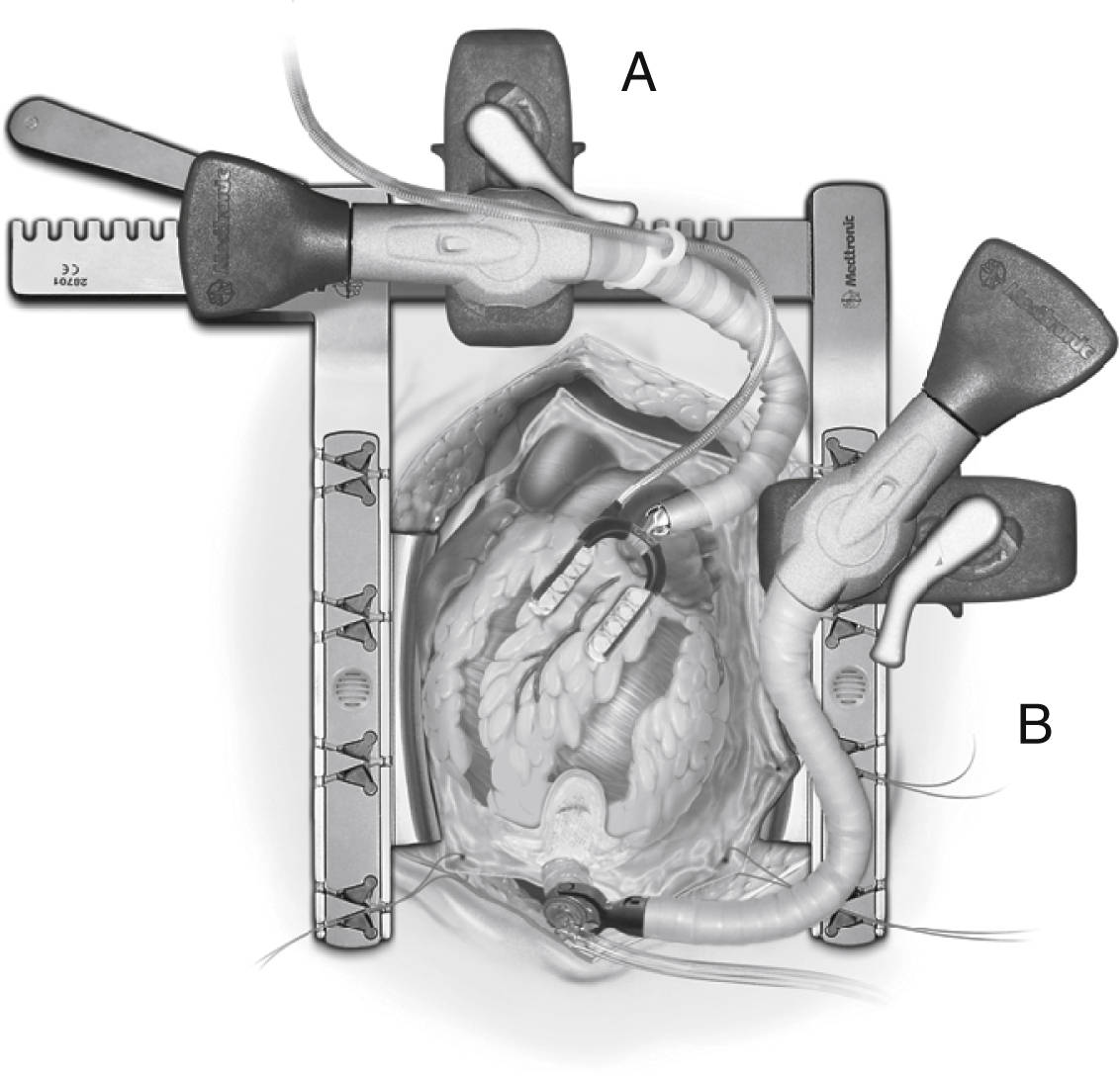
In operations that necessitate entry into the heart (valve repair or replacement), CPB is required for perfusion of the body while the heart is arrested and opened. During CABG, the procedure is performed on the epicardial coronary arteries that lie on the surface of the heart, not inside the heart. Coronary bypass surgery can be performed without the use of CPB (off-pump CABG), thereby avoiding the deleterious effects associated with extracorporeal circulation (see Table 35.4). Off-pump surgery may be feasible when pulmonary function is poor but LV function is not severely compromised, and access to the target coronary arteries does not require excessive manipulation of the heart.2,3 During off-pump procedures, the heart beats to perfuse the systemic, pulmonary, and coronary circulations. This beating heart surgery has been facilitated with the use of stabilizing devices that isolate and reduce the motion of the portion of the artery to be anastomosed (Fig. 35.9A). An attachment applies suction to the LV apex and allows the heart to be retracted for access to the lateral (i.e., obtuse marginal branches) and posterior (i.e., posterior descending or distal right coronary artery) portions of the heart (see Fig. 35.9B). Patient teaching considerations related to on-pump or off-pump surgery are listed in Table 35.5.
FIG. 35.9A, Octopus Evo AS off-pump cardiac stabilizer minimizes motion at the coronary anastomotic site. B, Starfish Evo suction positioning device attaches to the apex of the heart and exposes the lateral and posterior coronary arteries for bypass. (Courtesy of Medtronic Inc., Minneapolis, MN.)
Other technical advances have brought together interventional procedures and traditional surgical treatments. This combination is seen in the hybrid cardiovascular suite, which enables patients to receive both percutaneous coronary stent placement and traditional surgical revascularization. Additional hybrid cases such as percutaneous aortic and mitral valve procedures, pacemaker lead extractions, and percutaneous venous thrombus removal have not only expanded the indications for use of a hybrid room but have also brought together clinicians from the OR, cardiac catheterization and electrophysiology laboratories, and interventional radiology suites.10
Table 35.5
Patient Teaching Considerations for Minimally Invasive Surgery (On/Off Pump)
Beating Heart/Off-Pump
Arrested Heart
Definition
CABG without CPB or induced cardiac arrest; HR and contractile force may be pharmacologically reduced; stabilizer used at anastomotic site; apical retractor used to expose lateral and posterior coronary arteries
CABG with CPB and endovascular technique for CPB and induced cardiac arrest
Indications
Multiple-vessel disease, angioplasty contraindicated, medical problems, poor anatomy, accessible target arteries, previous CABG with blocked grafts
Multiple-vessel disease; angioplasty contraindicated, need to stop heart to enhance technical precision, accessible target arteries, mitral valve disease
Contraindications
Intramyocardial lesions, hemodynamic instability
High complex lesions, posterior targets
Incisions
Sternotomy or ministernotomy (cephalad or caudad); 1–3 small right or left, rib or submammary incisions
1–4 small rib incisions, 1 or 2 groin incisions
CPB
No, available on standby
Yes
Cardioplegia
No
Yes
Procedure time
2 hours or more
2 hours or more
Hospital LOS
3–5 days (versus 4–6 days for sternotomy)
3–5 days (versus 4–6 days for sternotomy)
Advantages
Avoids CPB, ischemic arrest, and hypothermia; may enable more complete revascularization with postoperative insertion of intracoronary stents into posterolateral coronary arteries in cardiac catheterization laboratory (hybrid procedure)
Allows repair of more complex lesions without technical challenge of moving heart; better ability to produce more complete revascularization
Potential complications and disadvantages
Learning curve technically more challenging; may cause VF; may have to revert to standard sternotomy with CPB and induced arrest
Learning curve technically more challenging; may have to revert to standard sternotomy; potential for endovascular injury to cannulated blood vessels
Discharge planning
Anticipated faster recovery of 1–2 weeks (versus 4–12 weeks for sternotomy), earlier ambulation, need to identify reportable signs and symptoms (angina, difficulty breathing, infection)
Anticipated faster recovery of 1–2 weeks (versus 4–12 weeks for sternotomy), earlier ambulation, need to identify reportable signs and symptoms (angina, difficulty breathing, infection)
Left Ventricular Aneurysm Repair
Repair of an LV aneurysm represents another form of myocardial revascularization in that the surgical remodeling of the LV by removing ischemic tissue status/post an MI improves coronary circulation and improves cellular viability. An LV aneurysm resulting from a large MI or numerous smaller adjacent infarctions causes a portion of the myocardial wall to become scarred, necrotic, thin, and weak. Scar tissue does not contract during systole but instead bulges outward (paradoxical motion or dyskinesia), which decreases the patient’s cardiac output (CO). Thrombus can form within the trabeculations of the LV, and pieces of thrombus can break off and embolize to the systemic circulation. In addition, the perimeter around the scarred fibrotic aneurysmal area can alter conduction pathways and create reentrant ventricular dysrhythmias. Surgical repair consists of excision of the aneurysmal tissue, removal of existing thrombus, and insertion of a patch into the LV in a manner that restores a more normal (i.e., elliptic) ventricular geometry. If the patient continues to have recurrent ventricular tachycardia, electrophysiologic mapping and possible insertion of an implantable cardioverter-defibrillator (ICD) may be performed after surgery in the electrophysiologic laboratory.3
Valvular Heart Surgery
Valve surgery is performed more commonly on valves in the left side of the heart (i.e., aortic and mitral valves), because the higher pressures on the left side aggravate traumatic, infectious, or other preexisting injury to the valves and valve components. Repair of the native valve is preferred to replacement when possible. A left heart catheterization yields information concerning the left atrium (LA) and ventricle, the proximal aorta, aortic and mitral valves, and the coronary arteries. Echocardiography increasingly is the gold standard for the diagnosis of valvular heart disease. Other imaging processes include aortography that displays the size and function of the aorta and can be used to identify the location of the intimal tear in a dissection. Computed tomographic (CAT) scan and magnetic resonance arteriography have largely replaced aortography for imaging of aortic disease.11
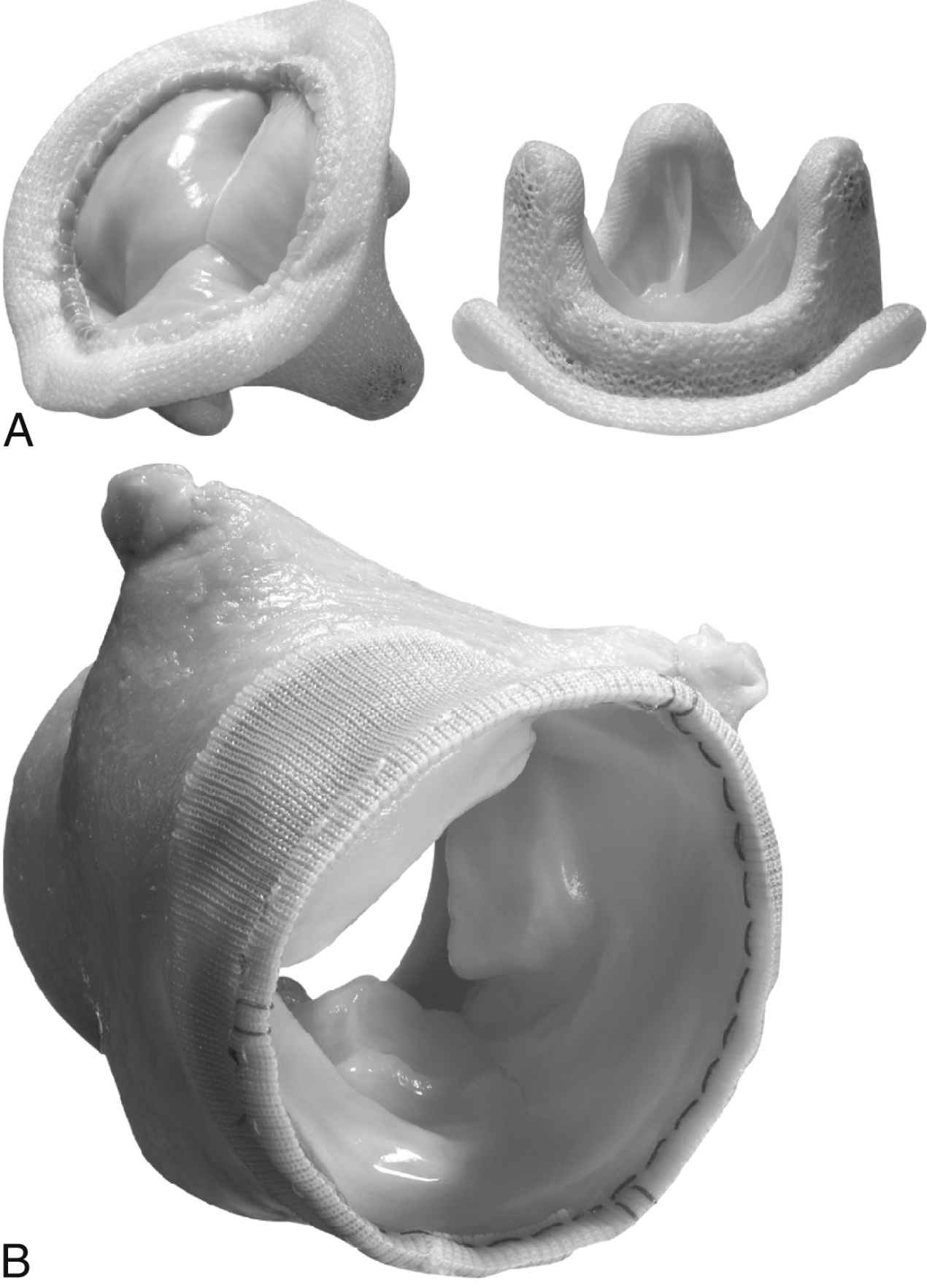
When surgery for valve replacement or repair is indicated, the surgeon selects and inserts the appropriate prosthesis. Valve replacement can be accomplished with biologic (Fig. 35.10) or mechanical (Fig. 35.11) prostheses. Newer percutaneous aortic valve prostheses (Fig. 35.12) are increasingly available primarily to patients who may be unable to withstand surgical replacement.12 Allografts (Fig. 35.13) can serve as biologic valve replacements. Allografts are advantageous because they do not require warfarin anticoagulation, are resistant to infection, and have excellent hemodynamics. They are also useful in patients with small aortic roots, because no sewing ring exists to decrease the size of the aortic valve orifice unlike prosthetic biologic or mechanical valves. Disadvantages include less availability and fewer technical difficulties associated with insertion. Bioprostheses have the advantage of not requiring chronic anticoagulation postoperatively unless there are other indications such as chronic atrial fibrillation (AF); their disadvantage is that they do not last as long as mechanical prostheses. Bioprostheses are stored in glutaraldehyde before implantation; the solution must be rinsed off the prosthesis usually in three baths of normal saline solution.
FIG. 35.10 Biologic valves. A, Medtronic Hancock II porcine bioprosthesis (side view and top view). B, Freestyle Aortic Root bioprosthesis. Stentless porcine aortic root bioprosthesis. Use of porcine stentless valves has reduced demand for cadaver allografts. These valves are especially useful in patients with small aortas. (Courtesy of Medtronic Inc., Minneapolis, MN.)
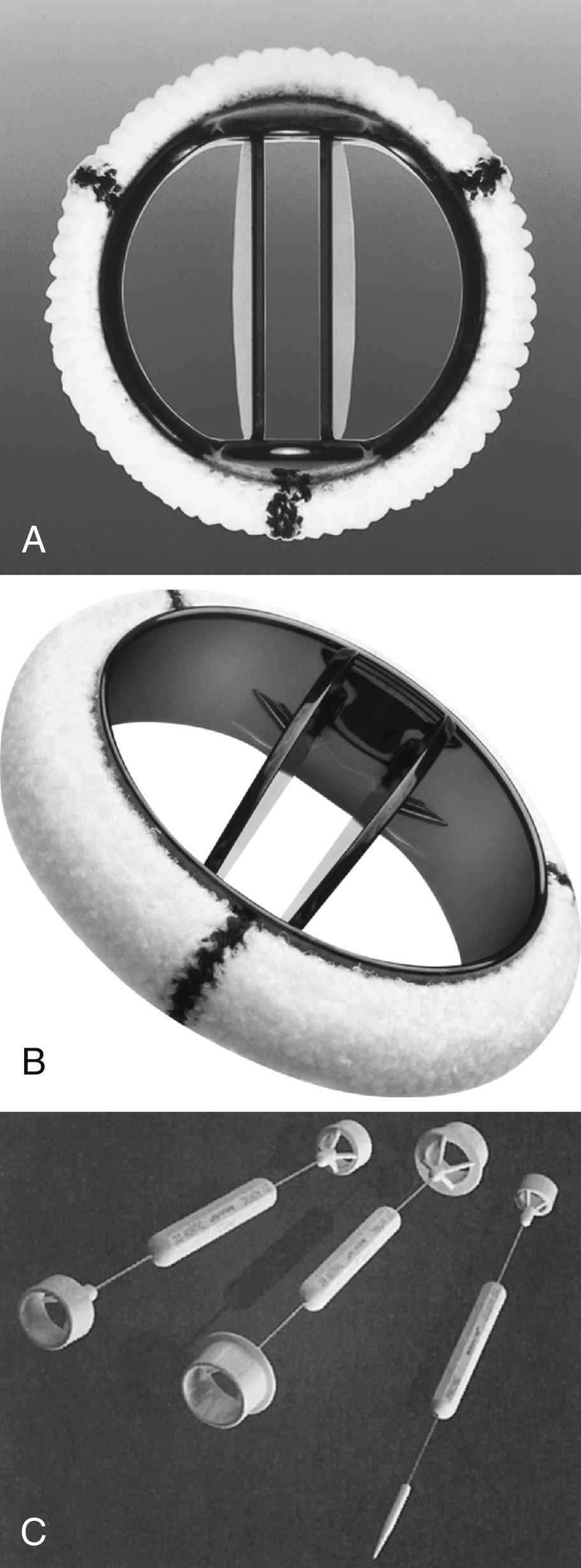
The advantage of mechanical valves is their durability. The disadvantage is that they require continuous anticoagulation therapy after surgery because mechanical prostheses are thrombogenic.
FIG. 35.11 Mechanical valves. A, St. Jude Medical bileaflet tilting disk valve prosthesis. B, Medtronic Open Pivot mechanical valve. C, Double-ended obturators (left and center) for sizing patient’s valve; probe (right) used to test prosthetic leaflet motion. Sizing obturators are specific to prosthesis. (A, Courtesy of St. Jude Medical, St. Paul, MN. B and C, Courtesy of Medtronic Inc., Minneapolis, MN.)
Only gold members can continue reading. Log In or Register to continue