11 Bursae Injections
Bursitis is commonly diagnosed and treated in clinical practices that focus on musculoskeletal medicine. Inflamed bursae often respond to conservative treatments including rest, cryotherapy, compression, physical/occupational therapy and nonsteroidal antiinflammatory drugs (NSAIDs).1a In patients who fail to respond to conservative rehabilitation, a corticosteroid injection into the bursa can serve as a useful diagnostic and therapeutic adjunct to a comprehensive course of rehabilitation.
Physical examination will reveal focal tenderness, swelling, and pain during direct palpation. If the injury is due to acute trauma, a fracture or ligamentous instability of the joint should be considered. In cases of chronic bursitis, calcifications may be identified on plain radiographs. However, the most common etiology combines repetitive motion with improper biomechanics. The physical examination should include a survey of peripheral joints to rule out a systemic process such as an underlying rheumatic disease. Skin overlying the area of tenderness should be examined for evidence of warmth, redness, swelling, or penetrating trauma. Rarely an infected bursa is diagnosed, and skin warmth appreciated on palpation may be the most sensitive physical indicator.1 The treatment of bursitis requires that an infection be considered prior to initiating treatment protocols. Aspiration of a septic bursa and identification of a bacterial pathogen are necessary to initiate appropriate antibiotic treatment. Laboratory studies of the serum should include an erythrocyte sedimentation rate, complete blood cell count, and microscopic examination to screen for leukocytosis, bacteria on Gram stain, or crystals. Operative incision and drainage of a septic bursa may be required for effective treatment.2,3 Contraindications to bursal injection with corticosteroids include cellulitis, generalized infection, and coagulation disorders.
Subacromial (Subdeltoid) Bursitis
The subacromial bursa rests on the supraspinatus and is covered by the acromion, the coracoacromial ligament, and the deltoid. This is the most common site of bursitis of the shoulder, with inflammation usually occurring secondary to rotator cuff tendinitis or shoulder impingement syndrome. In a pure subacromial bursitis, the impingement signs may be absent, and the inflamed bursa may limit full passive abduction due to compression at the near end range of shoulder motion.4 More commonly, subacromial bursitis coexists with impingement syndrome or rotator cuff syndrome. Determining the etiology of shoulder pain may be difficult, and a diagnostic injection into the bursa can narrow the field of possibilities. A diagnostic injection may help distinguish weakness and loss of range of motion secondary to a painful bursitis from a full-thickness rotator cuff tear. The patient should be thoroughly examined prior to the administration of local anesthetic and then reexamined 5 to 10 minutes after injection. Postinjection, the patient may be less guarded and more cooperative during the physical examination, yielding further diagnostic information.
Although an anterior, posterior, or lateral approach may be used, the posterolateral approach is preferred. Following sterile technique, the skin is cleansed with povidone-iodine, and the patient is directed to retract the shoulder to a neutral posture. The posterolateral angle of the acromion is identified by palpation, and the needle is advanced in an anteromedial and slightly inferior direction (Figs. 11-1 and 11-2).5 If the soft tissues resist needle insertion, a small volume can be injected to expand the bursa so that the needle can be advanced further, resulting in optimal needle position. A mixture of 2 to 4 mL of 1% or 2% lidocaine hydrochloride and 2 to 4 mL of 0.5% bupivacaine hydrochloride is injected into the bursa after a 25-gauge, 1.5-inch needle is introduced approximately 1 inch.6 In the authors’ experience, an inflamed subacromial bursa accepts 4 to 6 mL of total volume. Following the injection, a reduction of pain with improved strength supports the diagnoses of shoulder impingement, supraspinatus tendinitis, and subdeltoid bursitis. Patients who respond with greater than 50% relief are good candidates for an immediate follow-up injection with 1 mL of betamethasone sodium phosphate.6 Alternatively, the anesthetics can be mixed with the corticosteroids and administered in a single injection when the clinical examination is clear. Subacromial bursography is helpful when the initial blind anesthetic injection is unsuccessful or in a patient whose diagnosis is unclear. A normal bursogram casts doubt on a diagnosis of subacromial impingement.7

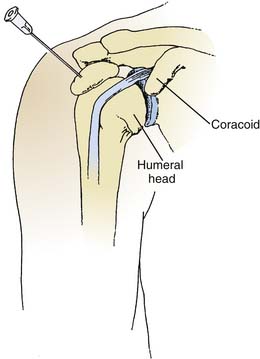
Figure 11-2 Schematic of subacromial bursa injection.
(Modified from Vander Slam TJ: Atlas of Bedside Procedures. Boston, Little, Brown, 1988.)
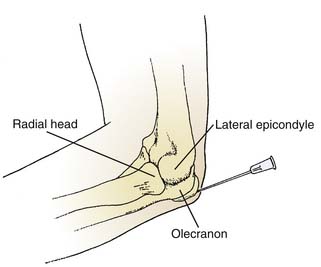
Olecranon Bursitis (Draftsmen’s Elbow)
The olecranon bursa is subcutaneous, protecting the proximal ulna frequently subjected to trauma. Inflammation of this bursa is commonly associated with rheumatologic disorders. Aspiration of the bursa should always precede injection and may be helpful to ensure proper location of the needle because the wall of the bursa is often thickened and fibrotic from chronic irritation. Gout may be seen at the olecranon, and any bursal fluid aspirated should undergo microscopic examination for crystals. Aspiration of the bursa is more successful using a larger bore needle (18 gauge), because the fluid may be gelatinous. The needle enters the skin perpendicular to the central swelling while the clinician withdraws on the syringe (Fig. 11-3).5 The procedure is followed with the application of a compressive dressing, and the patient is instructed to protect the elbow from further trauma. Persistent cases may benefit from a low-dose corticosteroid injection. Rarely, surgical excision or an arthroscopic bursectomy is warranted after failure of conservative measures.2