Chapter 20 Burns
Skin is the largest organ in the body, approximating 15% of body weight and 4.9 square metres in an adult. It has a number of functions, which correspond to the rationale of management and the potential complications of burns:
ASSESSMENT OF THE BURNS PATIENT
• History of the patient, including any chronic conditions that may affect wound healing such as steroid use, diabetes etc. Check tetanus status.
• Assessment of the depth and extent of the burn injury using standard protocols such as Wallace’s Rule of Nines or the Lund and Browder chart (Figure 20.1).
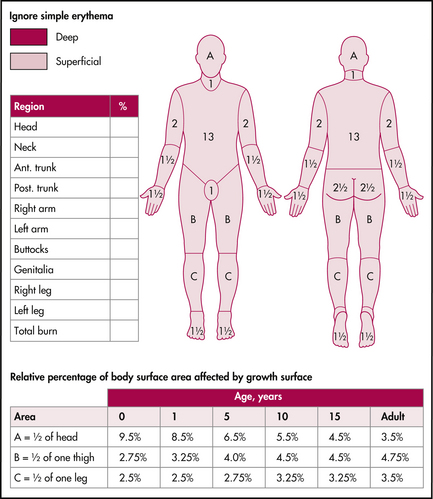
ASSESSMENT OF DEPTH AND EXTENT OF BURN
Depth of burn
The utilisation of terms such as first-, second- and third-degree has been largely replaced by:
• Superficial. Refers to epidermal reddening, e.g. sunburn. Extremely painful, no blistering, skin is red and heals spontaneously without scarring, usually within a week.
Note: Superficial burns are not counted in assessing the extent of burn injury.
• Partial thickness. Subdivided into superficial and deep:
• Superficial partial thickness—red or pink with mild blistering as involves dermis. Extremely painful but heals spontaneously within 1–2 weeks.
GENERAL MANAGEMENT
• Provide supplemental oxygen if there is any possibility of blast injury, smoke or toxic fume inhalations, stridor, hoarseness of the voice, burns to the face or any evidence of soot around the mouth or nose.
• Any burned patient removed from an enclosed space may be assumed to have airway injuries even when no burns are evident.
Analgesia
Superficial and partial thickness burns are extremely painful.
Simple oral analgesia may be required at home.
Inability to control pain is an indication for admission, particularly in children.









