BURNS
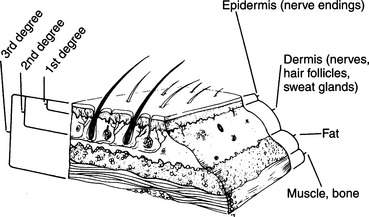
DEFINITIONS (Figure 93)
First-degree burn. This is a burn that involves the outermost layer of skin, the epidermis. It is often quite painful. The skin is reddened, but there is no blister formation. When a large surface area is involved, as with an extensive sunburn, the victim may become quite ill, with fever, weakness, chills, and vomiting.
Second-degree burn. This is a burn that involves the epidermis and portions of the next-deeper layer of the skin, called the dermis, which contains the sweat glands, hair follicles, and small blood vessels. It is usually more painful than a first-degree burn, and blisters are present. Large areas of second-degree injury impair the body’s ability to control temperature and retain moisture. Thus, a severely burned victim loses large amounts of fluid and can rapidly become hypothermic in a cold environment.
Third-degree burn. This is a burn that has penetrated the entire thickness of the skin, and may involve muscle, bone, and so on. It is typically painless because of nerve destruction. The appearance is dry, hard, leathery, and charred. Occasionally, the skin will appear waxy and white with small clotted blood vessels visible as purple or maroon lines below the surface. Because a third-degree burn is usually surrounded by an area of second-degree injury, the edges of the wound may be quite painful. Third-degree burns nearly always require a skin graft for coverage.
Partial-thickness burn. First-degree or second-degree burn.
Full-thickness burn. Third-degree burn.
Inhalation injury. This is a burn that involves any portion of the airway. Inhalation injury occurs when a victim is trapped in a fire and inhales smoke, steam, or superheated air (see page 114).
TREATMENT FOR BURNS
1. Remove the victim from the source of the burn. If his clothing is on fire, roll him on the ground or smother him in a blanket to extinguish the flames. Remove all materials that are hot or burned. If the victim has been burned with chemicals, gallons of water should be used to wash off the harmful agents. If chemicals may be present in an article of clothing, remove it. If the eyes are involved, they should be irrigated copiously. Phosphorus ignites on contact with air, so any phosphorus in contact with the skin must be kept covered with water. Do not attempt to neutralize acid burns with alkaline solutions or vice versa; the resultant chemical reaction may liberate heat and worsen the injury. Stick to irrigation with water. If clothing remains stuck to the skin and does not fall away with irrigation, do not tear the clothing away. Cut around it.
2. Evaluate the airway. Look for evidence of an inhalation injury: burns of the face and mouth, singed nasal hairs, soot in the mouth, swollen tongue, drooling and difficulty in swallowing saliva, muffled voice, coarse or difficult breathing, coughing, and wheezing. If it appears that an inhalation injury has occurred, administer oxygen (see page 431) by face mask at a flow rate of 5 to 10 liters per minute, and transport the victim to a hospital as quickly as possible.
3. Examine the victim for other injuries. Unless the airway is involved or the victim is horribly burned, the burn injury will not be immediately life threatening. In your eagerness to treat the burn, don’t overlook a serious injury such as a broken neck. Control all bleeding and attend to broken bones before applying burn dressings.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


