Chapter 17 Bronchoscopy
1 What is flexible bronchoscopy?
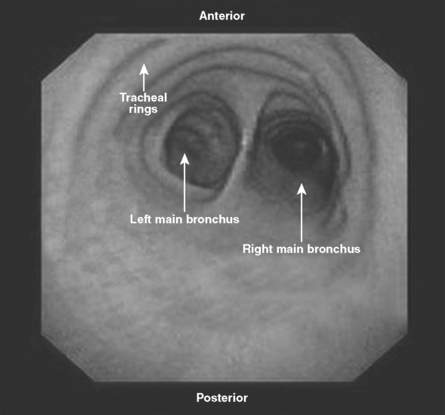
Bronchoscopy literally means “to see the airways.” This procedure allows visualization of the upper airways, trachea, and bronchi. Flexible bronchoscopy uses a small-caliber fiberoptic scope, which is passed through the nose or mouth or through a tracheostomy or endotracheal tube (Fig. 17-1). The bronchoscope is then directed down the trachea to the main carina (Fig. 17-2) and beyond to the regions of interest. In most patients, the airways can be visualized at least to the segmental bronchi.

2 How is flexible bronchoscopy performed?
1. Set up suction equipment and monitoring for cardiac rhythm, blood pressure, and oxygenation saturation. Supplemental oxygen should be provided via nasal cannula or face mask.
2. Numb the patient’s nose and pharynx with topical lidocaine.
3. Control cough and gag with small doses of short-acting narcotic and benzodiazepines.
4. Lubricate the bronchoscope with topical lidocaine jelly. Anesthesia of the posterior pharynx, vocal cords, and carinas is particularly important because advancing the bronchoscope past these areas is most likely to cause the patient to cough.
6 What are the indications for bronchoscopy in the intensive care unit (ICU)?
Bronchoscopy allows inspection of the airways, collection of samples from the lower airways, and performance of various interventions (Table 17-1). In the ICU, it is most commonly used to diagnose infection via bronchoalveolar lavage (BAL) or protected specimen brush. In BAL, the tip of the bronchoscope is wedged into a subsegmental bronchus while aliquots of saline solution (typically 30 mL each) are injected and aspirated into sterile traps. Alveolar contents are collected while the bronchoscope position prevents flooding of other regions of the lung. The protected specimen brush is a sterile brush with a gelatin cap that is inserted into a potentially infected area, agitated, then withdrawn and sent for culture.
Table 17-1 Indications for bronchoscopy
| Step | Indication | Goal |
|---|---|---|
| Inspection | Hemoptysis | Localize bleeding |
| Search for endobronchial lesion | ||
| Infection | Identify evidence of inflammation or pus | |
| Aspiration | Look for foreign bodies | |
| Mass | Look for endobronchial masses | |
| Chest trauma | Find evidence of airway injury | |
| Inhalational injury | Find evidence of airway injury | |
| Sample collection | Pulmonary infiltrates (infectious) | Obtain samples for Gram stain, silver stain, bacterial cultures, and viral and fungal studies |
| Pulmonary infiltrates (noninfectious) | Identify alveolar hemorrhage | |
| Check for eosinophilia (analyze cell count and differential) | ||
| Mass or adenopathy | Perform transbronchial biopsy for cytologic or pathologic analysis | |
| Interventions | Hemoptysis | Control bleeding |
| Bronchial obstruction | Remove mucus or foreign bodies | |
| Perform laser removal of masses | ||
| Place stent | ||
| Alveolar proteinosis | Perform lavage | |
| Intubation | Visualize anatomy for tube placement |



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


