CHAPTER 100
Boxer’s Fifth Metacarpal Fracture
Presentation
The patient seeks help for painful swelling of the hand over the distal fifth metacarpal (MC) after punching an object or another person with a closed fist. It occurs commonly during fistfights or from punching a hard object, such as a wall or a filing cabinet, and may be an act of deliberate self-harm.
What To Do:
 Obtain a clear history regarding the mechanism of injury and the circumstances that led up to the punching incident.
Obtain a clear history regarding the mechanism of injury and the circumstances that led up to the punching incident.
 Examine the patient’s hand, with attention to inspection and palpation of the fifth MC. The normal prominence of the fifth knuckle may be lost, and most often there will be tenderness at the neck of the fifth MC, where the shaft meets the head.
Examine the patient’s hand, with attention to inspection and palpation of the fifth MC. The normal prominence of the fifth knuckle may be lost, and most often there will be tenderness at the neck of the fifth MC, where the shaft meets the head.
 Obtain routine radiographs of the injured hand to determine the exact nature and degree of angulation of any fracture.
Obtain routine radiographs of the injured hand to determine the exact nature and degree of angulation of any fracture.
 Also, assess for malrotation by examining the direction of the fingers in flexion. All of the fingertips should be aligned parallel to one another (Figure 100-1).
Also, assess for malrotation by examining the direction of the fingers in flexion. All of the fingertips should be aligned parallel to one another (Figure 100-1).
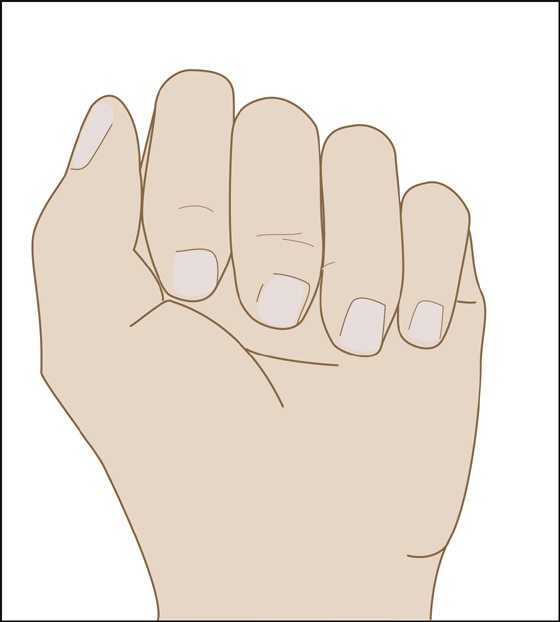
Figure 100-1 Normal alignment.
 No malrotation is acceptable. If any malalignment is present (Figure 100-2), inject the fracture hematoma with a long-acting local anesthetic (e.g., bupivacaine [Marcaine] 0.5%), and, with traction and counterrotation, reduce any malrotation. Buddy-tape the fifth finger to the fourth finger to maintain normal alignment.
No malrotation is acceptable. If any malalignment is present (Figure 100-2), inject the fracture hematoma with a long-acting local anesthetic (e.g., bupivacaine [Marcaine] 0.5%), and, with traction and counterrotation, reduce any malrotation. Buddy-tape the fifth finger to the fourth finger to maintain normal alignment.
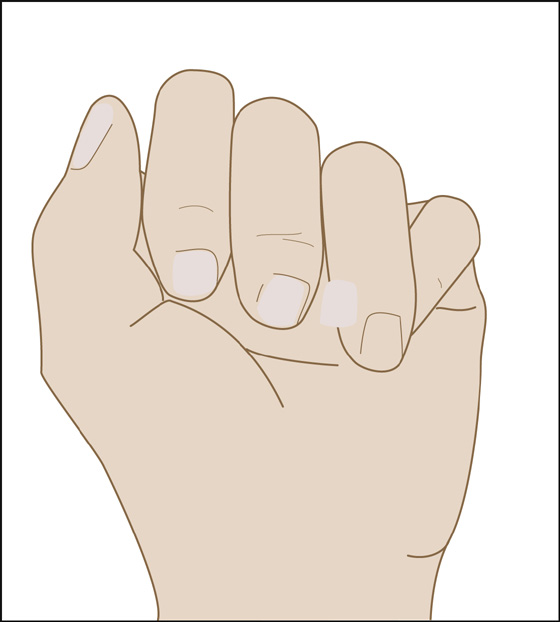
Figure 100-2 Rotational deformity.
 Most fractures occur just below the metacarpal head without rotation but are usually displaced in a volar direction. Up to 70 degrees of volar angulation is acceptable in the nonoperative management of a boxer’s fracture.
Most fractures occur just below the metacarpal head without rotation but are usually displaced in a volar direction. Up to 70 degrees of volar angulation is acceptable in the nonoperative management of a boxer’s fracture.
 Patients with a rotational deformity (with or without reduction) should be placed in an ulnar gutter splint with the fourth and fifth metacarpophalangeal (MCP) joints in a 90-degree flexed position and given orthopedic follow-up within 1 week.
Patients with a rotational deformity (with or without reduction) should be placed in an ulnar gutter splint with the fourth and fifth metacarpophalangeal (MCP) joints in a 90-degree flexed position and given orthopedic follow-up within 1 week.
 Patients with up to 70 degrees of volar angulation without rotation can be treated with a simple pressure bandage (e.g., bulky cotton padding wrap covered with an elastic bandage) along with adequate analgesics, such as acetaminophen alone or nonsteroidal anti-inflammatory drugs (NSAIDs) and/or hydrocodone/acetaminophen (Lorcet, Lortab, Vicodin).
Patients with up to 70 degrees of volar angulation without rotation can be treated with a simple pressure bandage (e.g., bulky cotton padding wrap covered with an elastic bandage) along with adequate analgesics, such as acetaminophen alone or nonsteroidal anti-inflammatory drugs (NSAIDs) and/or hydrocodone/acetaminophen (Lorcet, Lortab, Vicodin).
 After 1 week, these patients are allowed immediate mobilization within the limits imposed by pain.
After 1 week, these patients are allowed immediate mobilization within the limits imposed by pain.
 Self-harmers and patients who are having problems controlling their anger should be considered for psychiatric assessment and referral.
Self-harmers and patients who are having problems controlling their anger should be considered for psychiatric assessment and referral.
What Not To Do:
 Do not overlook a so-called “fight bite” injury. All open wounds over the MCP joints should be considered “fist-to-mouth” human bite wounds, which have the highest incidence of infectious complications of any closed-fist injury and of any type of bite wound (see Chapter 144).
Do not overlook a so-called “fight bite” injury. All open wounds over the MCP joints should be considered “fist-to-mouth” human bite wounds, which have the highest incidence of infectious complications of any closed-fist injury and of any type of bite wound (see Chapter 144).
Discussion
An isolated fracture of the distal fifth metacarpal bone, known as a boxer’s fracture, is the most common type of metacarpal fracture. Boxer’s fractures received their name from one of their most common causes—punching an object with a closed fist. This is somewhat of a misnomer, because boxers learn not to punch this way, and the injury is seen more commonly in a lay person striking a hard object with a closed fist.
Reduction of angulated fractures of less than 70 degrees appears to be of no value with respect to range of motion (ROM) of the fifth MCP joint. Patients with less than 70 degrees of volar angulation and no rotational deformity who were treated with a pressure bandage for 1 week, followed by immediate mobilization, showed no statistical differences with respect to ROM, satisfaction, pain perception, return to work/hobby, and need for physiotherapy when compared with patients treated for 3 weeks with a plaster ulnar gutter splint.
This injury has been described as “a tolerable fracture in an intolerable patient.” Anxiety symptoms and maladaptive personality traits are very common in patients with boxer’s fractures. Psychiatric assessment and counseling should be strongly considered in these patients, who actually have a high risk for recurrence of self-harm or aggressive acts.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


