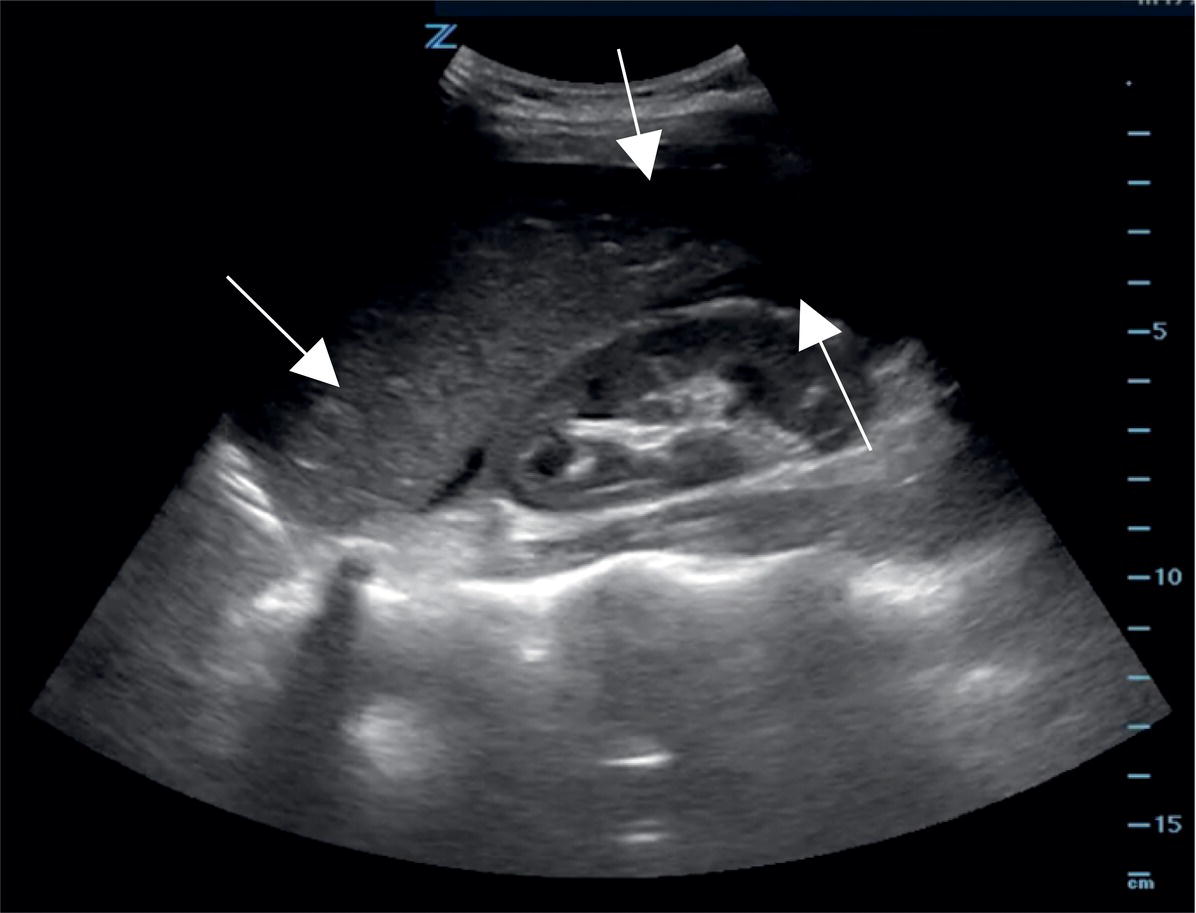
Brendan M. Carr and Fernanda Bellolio Department of Emergency Medicine, Mayo Clinic, Rochester, MN, USA In the acutely injured patient with abdominal trauma, several diagnostic modalities are available in the emergency department (ED) to detect the presence of solid organ injury and intra‐abdominal hemorrhage. Many studies have compared abdominal ultrasound with computed tomography (CT) scan, most of which have shown that CT is superior to ultrasound in detecting intra‐abdominal injuries. A challenge often encountered with CT imaging in trauma patients, however, is that it cannot always be safely performed in unstable patients. In such patients, a diagnostic peritoneal lavage (DPL) performed at the bedside in the ED was historically the test of choice to assess for intra‐abdominal injury (e.g., hemorrhage, perforated viscus) for which surgical intervention may have been needed. In DPL, a surgical incision is made in the abdomen which is then lavaged for the presence of blood or red blood cells. In recent years, however, diagnostic ultrasound has emerged as a safe, rapid, and noninvasive alternative to DPL, and has replaced the use of DPL in hospitals at which ED ultrasound is available (Figure 8.1). The focused assessment with sonography for trauma (FAST) exam is the best‐studied and most commonly performed ultrasound protocol for trauma patients in the ED and will be the focus of discussion here. While the FAST exam is not 100% sensitive and thus cannot completely rule out the presence of intra‐abdominal injuries, it can be used during the initial evaluation of trauma patients to provide early information and rule in intra‐abdominal bleeding. Figure 8.1 A focused assessment by sonography in trauma (FAST) reveals fluid in Morison’s pouch and surrounding the caudal tip of the liver (arrows). (Courtesy of Tobias Kummer, MD.) How accurate is FAST compared to CT scan and DPL in adult patients with blunt abdominal trauma? One of the earliest prospective studies to compare DPL, the abdominal windows of the FAST exam, and CT scan was performed in China in 1990.1 Liu et al. compared the accuracy of the three modalities for the detection of significant intra‐abdominal injuries. Patients with stable vital signs after their initial resuscitation and who had equivocal physical examination findings underwent CT and ultrasound, followed by DPL. If any of the three exams were positive, the investigators performed a laparotomy. They compared surgical findings (the criterion standard) to the results of the diagnostic tests. For the 55 patients included in this early study, the sensitivity, specificity, and accuracy are shown in Table 8.1. Table 8.1 Early study of sensitivity and specificity of test sensitivity, specificity and accuracy of computed tomography (CT) scan, diagnostic peritoneal lavage (DPL), and ultrasound in 55 patients using surgical findings as the criterion standard Source: Data from Liu et al. [1]. Since then, many studies have been performed evaluating the use of ultrasound in adults with blunt abdominal trauma. A systematic review in 2012 evaluated the test characteristics of bedside FAST exam for “clinically significant intra‐abdominal injuries.” This reported a sensitivity and specificity of 74% and 96%, respectively, when the possibility of publication bias was factored into the calculations.2
Chapter 8
Blunt Abdominal Trauma
Background
Clinical questions
Sensitivity, %
Specificity, %
Accuracy, %
CT
97.2
94.7
96.4
DPL
100
84.2
94.5
Ultrasound
91.7
94.7
92.7
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


