Figure 16.1 Bladder imaging, transverse view. (a) Transducer placement with the indicator oriented towards the patient’s right side. (b) Anatomy, depicting the bladder and rectum. (c) Transverse ultrasound image of the bladder. Of note, it is important to angle the image beam down into the pelvis to obtain a proper image. (d) Corresponding illustration depicting major structures visualized including bladder and rectum. Illustration by Laura Berg, MD.
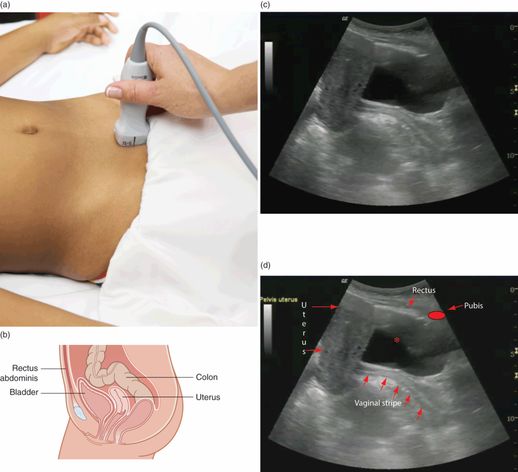
Figure 16.2 Bladder imaging, sagittal view. (a) Transducer placement with the indicator oriented towards the patient’s head. (b) Anatomy, showing the bladder, rectum, and uterus in a female patient. Artwork created by Emily Evans © Cambridge University Press. (c) Sagittal ultrasound image of the bladder. (d) Structures visualized: the bladder (*), pubis, uterus, vaginal stripe (arrows), and rectus muscle.
Technique
Transducer selection and orientation
A curvilinear transducer with an effective frequency of 2–5 MHz is used to visualize the bladder (Figure S3.3b). The bladder is imaged in two planes: transverse, with the indicator oriented towards the patient’s right (Figure 16.1a), and sagittal, with the indicator oriented towards the patient’s head (Figure 16.2a).
Patient position and preparation
For the point-of-care bladder ultrasound evaluation, the patient should be lying supine. When considering a suprapubic aspiration or catheterization, appropriate preparation must be performed, including the sterile preparation of the transducer (Figures S3.5–7), and of the patient’s skin. It is important to appropriately restrain the child, holding him/her in a frog-leg position (Figure 16.3).

Figure 16.3 Proper frog-leg positioning of a patient for bladder catheterization and suprapubic aspiration.
Ultrasound imaging
First, locate the pubic symphysis by manual palpation of the lower abdomen. Place the transducer midline, immediately superior to the pubic symphysis. Then, gently push down and slowly angle the transducer towards the patient’s feet, directing the beam into the pelvis (Figure 16.1a).
When full, the bladder should appear on screen as a trapezoidal anechoic structure with a surrounding thin, smooth, echogenic wall (Figures 16.1c,d and 16.2c,d). Once the transverse view is obtained, rotate the transducer clockwise 90°, with the indicator oriented towards the patient’s head in order to obtain the sagittal view. Again, push down gently and slowly angle the transducer slightly into the pelvis, pointing the beam towards the feet (Figure 16.2a). The bladder should be easily visualized when full. In contrast, an empty bladder may be difficult to visualize. The importance of obtaining two views of the bladder (transverse and sagittal) cannot be emphasized enough. However, the order in which these two views are obtained is up to the operator’s preference.
Ultrasound-guided procedure
Place the curvilinear or phased-array transducer just above the symphysis pubis and obtain both the transverse and sagittal views of the bladder. One may calculate bladder volume manually or as part of the machine’s calculation software. Alternatively, a novel single measurement has been utilized. Witt et al. utilized a single measurement of the transverse bladder diameter of greater than 2 cm as correlating with a sufficient volume for catheterization.
The formula for the calculation of bladder volume was derived from estimation.
One may assume that the bladder is similar to a sphere or a rectangle. Patients show variation in the shape of their bladder. Further, bladders with smaller volumes assume a trapezoidal shape, while those with larger volumes assume a more spherical shape. Therefore, the formula obtained takes into account these features with a correction factor of 0.75 (Figure 16.4). Note that different references use a slightly different correction factor, but the correction factor of 0.75 is the most widely used. Utilizing this formula correlates well with catheterized specimens. Of note, it is important to obtain measurements in centimeters, since the resulting cubic centimeters (cm3) are equivalent to milliliters (mL). This can be compared to the volume of urine expected for a particular age calculated by the equation:
Any volume greater than 3 cm3 will usually be adequate for specimen collection in 98% of catheterized patients.
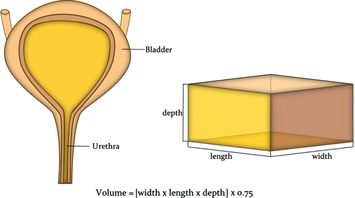
Figure 16.4 Calculation of bladder volume. An estimate of bladder volume may be calculated using the formula for a cube. However, since the bladder is more similar in shape to a sphere, a correction factor of 0.75 needs to be incorporated into the formula. Bladder volume = ([width × length × depth] × 0.75). This formula has been shown to correlate well with volumes obtained from catheterized specimens.
There are two methods of calculating the bladder volume: manually or via the machine’s automated calculation.
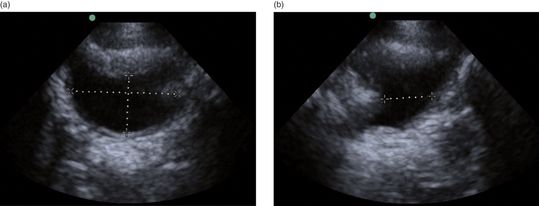
Figure 16.5 Bladder volume is calculated by making three measurements: width, height, and depth. (a) First the transverse image of the bladder is obtained (with the indicator oriented towards the patient’s right) and its height and width are measured. (b) The transducer is rotated with the indicator positioned towards the patient’s head. The additional measurement of depth may be obtained. Of note, some machines have automated programs, which will calculate the bladder volume when the operator inputs these measurements.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


