Chapter 37 Bioterrorism
2 What are some possible agents that might be used in an attack?
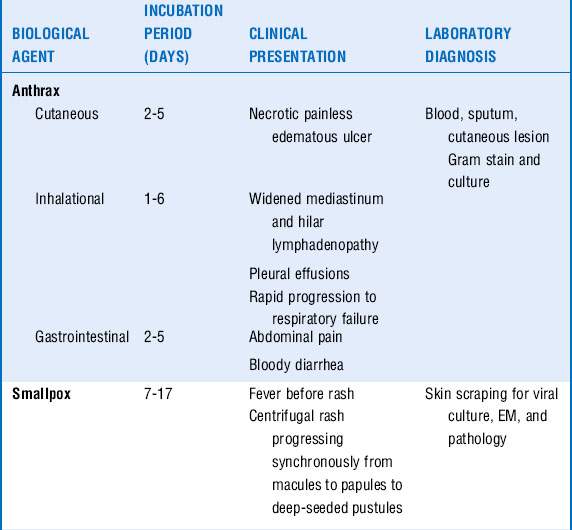
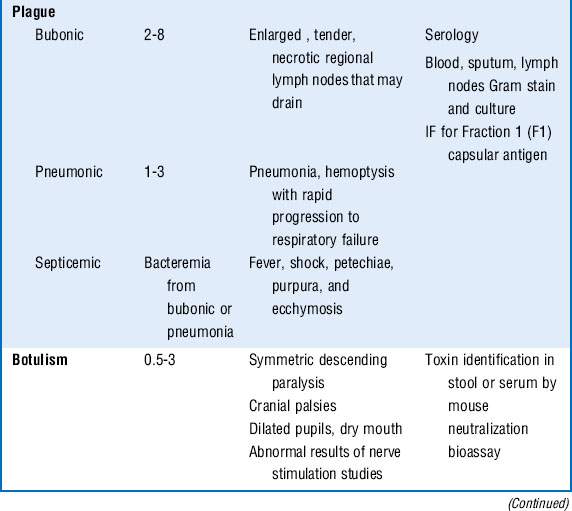
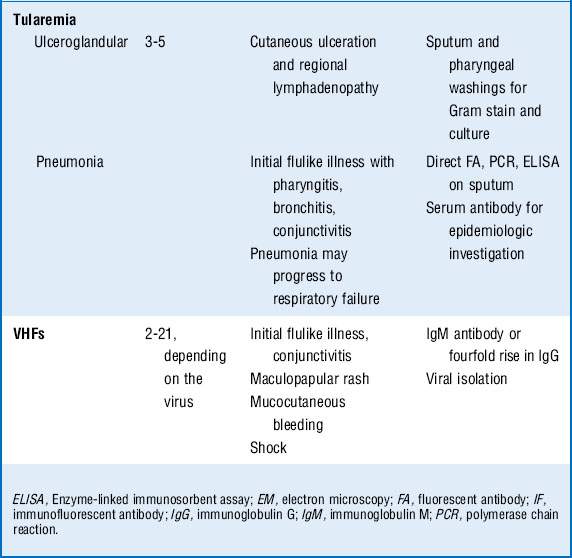
The CDC classifies six pathogens as class A bioterrorism agents: smallpox, plague, botulism, tularemia, viral hemorrhagic fever (VHF), and anthrax. These agents are considered to have the greatest potential for mass casualties, large-scale dissemination, and public panic and social disruption. All of them except VHF have been developed as biological weapons. They are stable in aerosol form and would be most likely delivered in this manner. Most of the civilian population remains susceptible to them, and most cause illnesses not typically seen by providers, causing delayed or missed diagnoses. The major clinical syndromes are summarized in Table 37-1.
3 What are clues to a biological attack?
Recognition of a biological attack may be delayed until patients begin accessing medical care, which may be days to weeks after the event depending on the incubation period of the pathogen (Table 37-1). Features that might suggest a biological attack include the following:






4 What pathogens would present with respiratory failure?
 Anthrax: Pneumonic anthrax is caused by the inhalation of the spore form of Bacillus anthracis. It begins as a nonspecific influenza-like illness with fever, cough, malaise, headache, and vomiting. Rapid progression occurs to hemorrhagic mediastinitis, hilar lymph node enlargement, respiratory failure, hemodynamic collapse, and death. Although chest radiographs classically show only a widened mediastinum without pulmonary infiltrates, several of the victims from the anthrax letter attacks in the fall of 2001 did have pulmonary infiltrates and pleural effusions. Bacteremia and meningitis can occur.
Anthrax: Pneumonic anthrax is caused by the inhalation of the spore form of Bacillus anthracis. It begins as a nonspecific influenza-like illness with fever, cough, malaise, headache, and vomiting. Rapid progression occurs to hemorrhagic mediastinitis, hilar lymph node enlargement, respiratory failure, hemodynamic collapse, and death. Although chest radiographs classically show only a widened mediastinum without pulmonary infiltrates, several of the victims from the anthrax letter attacks in the fall of 2001 did have pulmonary infiltrates and pleural effusions. Bacteremia and meningitis can occur.


5 What pathogens would present with shock?


7 What pathogens may present with predominantly cutaneous manifestations?
 Smallpox, caused by the DNA virus variola major, is acquired via inhalation of infectious droplets aerosolized by affected patients. Typically a prodrome of fever, chills, myalgias, and headache occurs over 2 to 4 days, followed by the eruption of intraoral macules. A maculopapular rash develops on the face, which then progresses in a centrifugal manner to involve the extremities and finally the trunk. The rash progresses to deep-seated vesicles and pustules over 8 to 10 days. Complications include bacterial superinfections, fluid and electrolyte abnormalities, desquamation, panophthalmitis, residual scarring, and death. Secondary bacterial infections involving the skin or lungs may occur and are often complicated by bacteremia and sepsis.
Smallpox, caused by the DNA virus variola major, is acquired via inhalation of infectious droplets aerosolized by affected patients. Typically a prodrome of fever, chills, myalgias, and headache occurs over 2 to 4 days, followed by the eruption of intraoral macules. A maculopapular rash develops on the face, which then progresses in a centrifugal manner to involve the extremities and finally the trunk. The rash progresses to deep-seated vesicles and pustules over 8 to 10 days. Complications include bacterial superinfections, fluid and electrolyte abnormalities, desquamation, panophthalmitis, residual scarring, and death. Secondary bacterial infections involving the skin or lungs may occur and are often complicated by bacteremia and sepsis.


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


