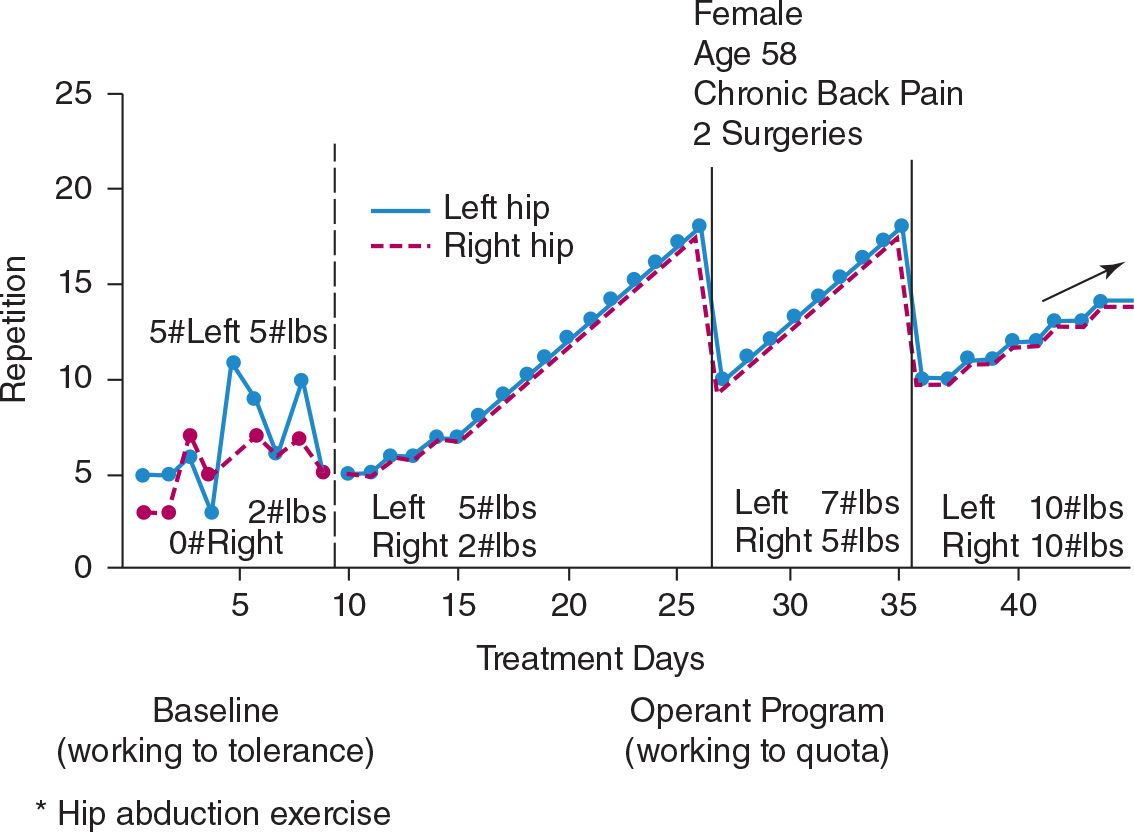
FIGURE 1 Recording exercise quotas and performance.
Diaries. Diary forms will have already been completed during the preadmission evaluation phase and so will be familiar. Diary recording continues in the same fashion, although a new diary form is begun on the day of admission.
Performance records. Each exercise and other treatment activity prescribed for the patient heads a column of the performance records. Rows correspond to treatment sessions. For the first day or two as each exercise is completed, the therapist can help the patient to record the amount accomplished before proceeding to the next exercise or procedure. During baseline trials the amounts accomplished represent a measure of current tolerance. Later, performance is recorded as amount done and the quota to which it relates. For example, if the exercise of deep knee bends has reached a quota of 12 and the quota is met, the proper cell of the form shows 12/12. If the quota was failed and only 10 were achieved, 10/12 would be recorded. Exercises involving pulling weights record the weight; for example, 9/9, 5 pounds. Exercises in which the left and right upper or lower extremity perform separately should also be recorded and graphed separately. Recording left and right separately has several advantages. The principal gain is that it permits one to identify and record differential performance between the left and right side. It also makes it easier to portray different quotas and quota-increment rates when that applies. Figure 2 describes such an instance. As shown in the baseline values, there was considerable disparity between her left and right hips on the abduction exercise. In the earlier phases of treatment, one side worked to move heavier weights than the other, although the number of repetitions and the increment rate were the same. Eventually the weaker side improved to where the therapist brought the two quotas into alignment. Performance of the two hips are shown in the figure as superimposed on each other to display the quota differences more clearly. In practice, the right and left graphs were maintained separately.
As was discussed in Chapter 10 on management of exercise, prescribed exercises must be quantifiable in performance terms. This issue sometimes requires careful review of therapist procedures. It is a point that is not always well understood. Working at a loom or with wall weights is not to be measured in time units but in numbers of units of completed performance: rows of weaving at a given width or repetitions at a given weight.
Many physical therapy exercises involve lifting or holding against weights of varying magnitude. Graph recording of performance for such exercises should reflect both the number of repetitions and the amount of weight against which force is exerted. Figure 2 illustrates the scalloped effect produced by such graphs. It will be noted from Figure 2 that the therapist’s initial quota began with the weights used in baseline trials. The disparity between left and right sides continued for some time before quotas were equalized.
There may be two potential exceptions to the performance-versus-time rule, but they may arise only in later stages of treatment after considerable progress will have occurred. The first exception relates to job station assignments. It is often difficult and logistically impractical to develop precise movement cycle units for job stations. Output and progress at the job station would be better monitored and rate of improvement would probably accelerate if the time were taken to analyze jobs in those terms. But that is often impractical. A compromise that can be hazardous is to record job station activity in time units. If review of a job station assignment indicates a reasonably steady rate of the job activity, performance may be recorded in time units. Should monitoring of job station performance suggest a general lagging of patient effort, the additional step of developing measurable production units should be resorted to. When that is done, the usual quota procedure can be applied. In noting this exception, it should be remembered that job stations enter into the picture only after there has been considerable patient progress in a range of activities all having quantifiable movement cycles. This point is important because it means that rest and attention will have been made contingent on performance, not time, and will have brought the patient to a point of intermittent and diminishing rates of reinforcement. At that point, the time method, a fixed interval schedule, is appropriate. The behavior has been established and rehearsed. Interval schedules tend to yield durable behavior, although they are less effective in generating a behavior. A similar exception was noted on p. 311 in relation to cooking or homemaking activities in occupational therapy. The exception is justifiable only after considerable treatment progress has occurred.
Graphs. The performance figures shown throughout the book were prepared from patient performance graphs. At the close of the baseline period, graphs can be posted at the bedside, and the transfer of data from performance records to graphs should begin. Graphing is not begun before that time because to do so would risk adding social reinforcement as a systematic consequence to performance during the baseline trials. Those baseline trials are strictly for the purpose of determining patient performance when he or she is left free to respond to inner cues or subjective experience.
Most professionals have at least some experience at constructing and reading performance graphs. Many patients do not have that experience. It is therefore important to follow up the initial instruction as to how to transfer performance data to graph form. After the first postbaseline treatment day, someone should go through the process with the patient to be sure the graphs are constructed properly. This first session of graph construction should include retroactive graphing of baseline trials, followed by display on each graph of the first quota or treatment sessions. Subsequently, daily ward rounds provide built-in monitoring of upkeep of graphs.
Graphs should be posted in a fashion that permits extension of performance of each procedure onto second and subsequent graph forms as they are needed. The display of a row of walking performance graphs from baseline tolerance trials, perhaps describing ability to go no more than a few hundred feet before resting to topped-off quotas of up to 1 or 2 miles, can provide an intensely rich reinforcement to patient, family, and staff.
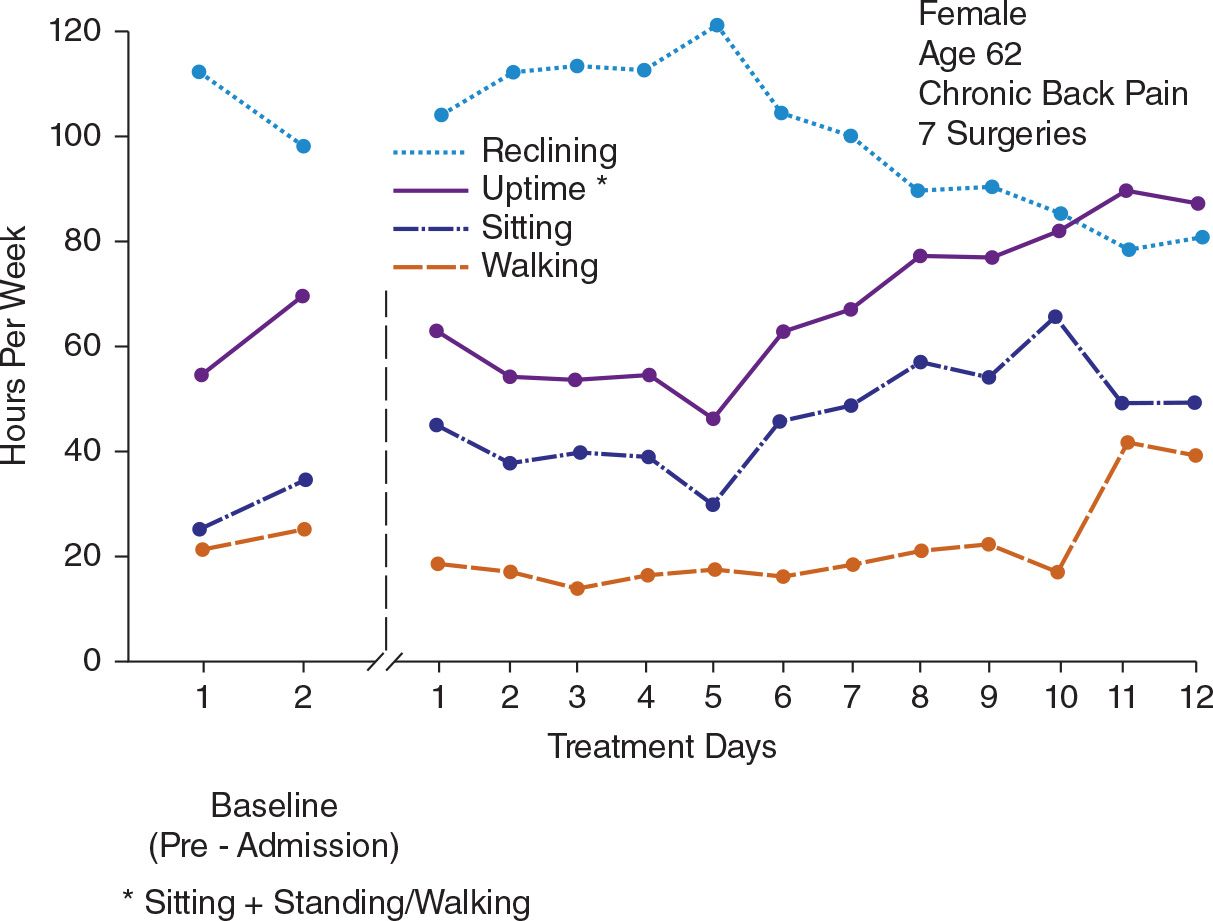
General activity level as recorded in diary forms should also be displayed in graph form for both daily and weekly units. The graph showing weekly cumulative uptime (sitting plus standing or walking) is often one of the most readable indices of patient progress, particularly when it displays preadmission performance, the week of baseline observations, and subsequent achievements.
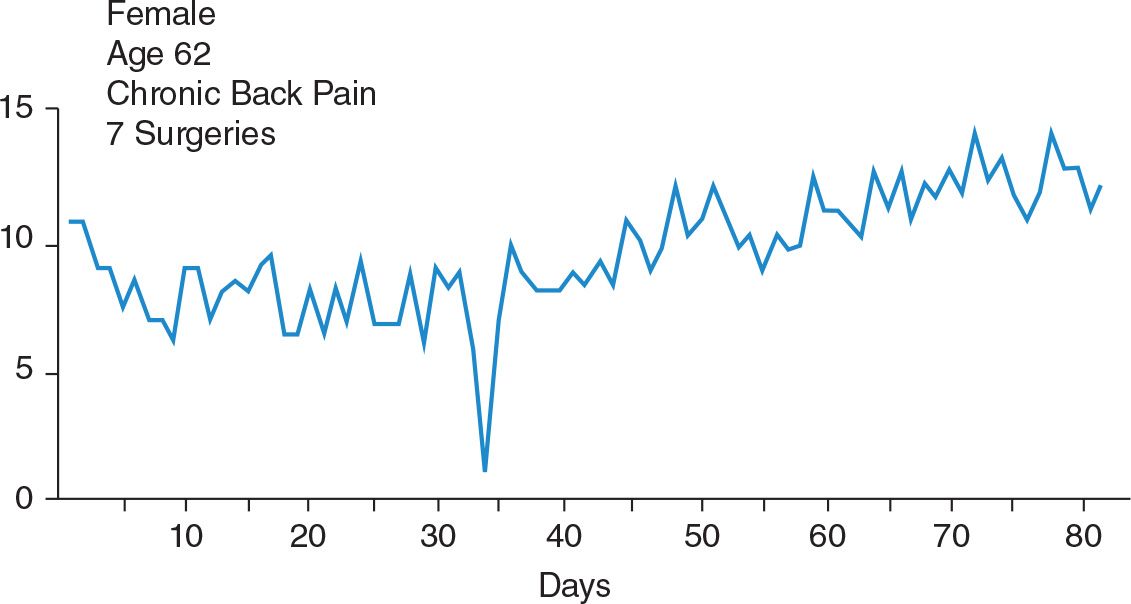
Figure 3 shows daily uptime totals for one severely impaired patient who had had seven surgeries and many significant neuromuscular deficits associated with those procedures, as well as severe distress from pain. Figure 4 reports the weekly totals from the same patient’s diaries of sitting, standing or walking, reclining, and the sum of sitting and standing or walking: uptime. There are several things to be noted about these figures. The daily uptime totals reflect the gradual trend upward of her activity level, but it is difficult to discern the extent to which she changed. The second graph, Figure 4, which reports weekly totals of each of the kinds of activities, yields both a more evident and a more precise picture of where the changes are occurring. Keeping the daily uptime graph helps the patient to focus attention on activity level. Keeping the weekly totals graph makes the major trends more evident and shows the changes from preadmission data to the present. Finally, this patient was severely involved. It was a long and arduous task for her to reach a significantly higher level of performance. Most patients will show changes in activity level sooner than those shown in Figure 4. The patient discussed on p. 226, whose weekly uptime totals were shown in Figure 3–3, represents one of the more rapid rates of increase in activity level.
One person within the treatment facility should be designated as the source for replenishment of diary and graph forms. The patient can then assume the responsibility for going to that person to receive additional performance, diary, and graph forms, as needed.
Reinforcement function of graphs. Reinforcing functions of graphs can be listed briefly.
1. Graphs provide rapid and precise report of performance, permitting patients to make more sensitive judgments of change.
2. Graphs help patients more precisely to communicate to spouses and others what is being accomplished in treatment.
3. Graphs provide reinforcement to spouse and other family members for their efforts in behalf of the program. These records of change often pick up progress more rapidly than casual observation.
4. Graphs demonstrate to treatment personnel whether their efforts are having an effect. Upward curves on graphs are tangible demonstrations of the effectiveness of therapist effort as well as that of the patient.
5. Graphs have indirect as well as direct reinforcing functions. When displayed prominently, graphs provide cues to people interacting with the patient to be prudent about the use of attention and social responsiveness. Graphs remind visitors, professional and nonprofessional, to be selectively responsive and also provide them with information about activity or well behavior to which they can respond.
MEASUREMENT OF PROGRESS (AND OF PAIN)
On pp. 29 and 30 there was a limited discussion of the measurement of pain. It was noted there that this book would not offer definitive measures of pain. The present chapter is concerned with procedural and not theoretical matters, but since the recording of progress and change is being discussed, a few additional comments about the matter of pain measurement are in order.
The procedures described here measure what people do who are identified as having functional limitations associated with chronic pain. If it is assumed that pain is an inner event, a subjective experience whose presence or absence depends on the verbal report of the person, the procedures described here do not measure pain. They do measure aspects of what the person does who has the pain problem. More particularly, these measurement procedures record changes in what the person does of those behaviors identified at the outset as limited by the pain problem. When the activities recorded (for example, diary data or exercise performance) indicate change, it is moot as to whether pain has changed, as well. Sometimes patients continue to state that the pain is unchanged. They are not surely correct. They may or may not be. The only data are patient statements about an alleged or inferred inner event. Similarly, patients may state that the pain is now improved or has disappeared altogether. That, too, may or may not be a correct statement.
The contingency management approach to chronic pain works with what people do, their actions or behavior. It is true that some attention is directed toward modifying what patients say about their pain. Those efforts necessarily lack precision and therefore lack as much effectiveness as other elements of the program. They are not intended to change anything more than what is said. It is not contended that helping a person to change what he or she says about pain changes inner, subjective experience.
What this comes down to is that the methods described in this book are directed at what people do. The measures used record changes in what they do. The behaviors of concern relate to reported pain problems, but it is not known whether behavior changes produced represent changes in unobserved and unmeasured inner events such as subjectively experienced pain.
SPOUSE AND FAMILY TRAINING
The procedures described in this section are for use with the spouse or whatever other person may be indicated. The person is selected who has played and is likely to continue to play a significant role in the direct or indirect reinforcement of pain behavior or the discouragement or punishment of activity and well behavior. The recipient of training is nearly always the spouse. Sometimes other family members such as a parent or in-law living within the home or adolescent or older progeny also participate. Occasionally, when the patient is unmarried, a girlfriend or boyfriend participate.
The social responsiveness of others as an important element in the picture usually relates to but one key person. Modification of that one person’s behavior in relation to the pain problem usually suffices. Typically the contributions of others are peripheral and, if warranting action at all, may be accomplished with a single contact or by preparing the spouse (or other key person) to be the agent for change of these others. The procedures to be described are presented with the spouse as the key person.
Some member of the treatment team with interviewing and interpersonal skills as well as knowledge of the operant program’s methods should be selected to carry out spouse training. In multidisciplinary hospital settings this might be a psychologist, psychiatrist, social worker, nurse, or some other health care professional. Selection is a matter of judgments about knowledge, skill, and interest, not professional identity.
Training procedures will need to be scheduled with a number of factors in mind. Assuming that the spouse or other recipient of the training is within reasonably easy commuting distance of the treatment setting, sessions probably should start with twice-weekly contacts of 20 to 40 minutes each. As progress occurs, the frequency can usually be reduced to once-a-week sessions.
Due allowance must be made for other commitments of the spouse. On the one hand, the procedure is clearly an integral part of treatment. The sessions should have been made an explicit requirement. Failure to agree to this participation ordinarily should result in refusal to accept the patient for treatment. On the other hand, scheduling should interfere as little as possible with the spouse’s employment and family responsibilities. Sessions may have to occur in the early or late parts of the day, as well as perhaps evenings or weekends. Those details need to be agreed on before treatment begins.
The operant program is specialized. Patients often come from great distances, far beyond commuting distance. In those cases, it is imperative before beginning treatment to clarify both the scheduling and the funding of spouse contacts. Special negotiations with third-party treatment sponsors may be required to get them to recognize that spouse visits are an integral component of treatment, without which the whole enterprise may be fatally compromised.
The spouse who must come from afar will require a different schedule pattern. The minimum indicated by clinical experience is that the spouse come with the patient at time of admission, remain for 1 to 3 days, return at least once during the inpatient phase for 2 to 3 days, and return again for approximately a week during the last part of the outpatient phase. Daily spouse contacts should be scheduled during that outpatient week.
Ideally, the spouse who lives at a distance should be seen each 2 or 3 weeks. He or she may come for a late afternoon session, visit the patient that evening, and have another training session the next morning before departure for home.
Concomitant with modification of spouse responses to pain behavior and to activity, the treatment program may use these sessions to help plan posttreatment activities. Joint sessions with patient and spouse should be scheduled for that purpose. In addition, problems indirectly related to the pain problem may also become a focus of spouse contacts. For example, a patient’s pain may yield time out from activities that, were they engaged in, would lead to marital strife. Spouse training sessions might then also have the character of marital counseling. The choice depends on whether these other problems are to be dealt with by the immediate treatment team. If they are to be treated by adjunctive therapists, that enterprise should proceed apace and with intercommunication with the treatment team.
It is of utmost importance to provide for coordination between the person working with the spouse and the rest of the treatment team. For example, evening visits, recreational activities, and weekend passes often involve the spouse. Those activities provide opportunity to rehearse steps in the training process. The activities must be made available at the proper times.
Pinpointing Target Behaviors
In consultation with the spouse, a list of pain behaviors that the patient displays with some frequency is identified and written out. These are the ways in which the spouse is made aware that the patient has a pain problem or functional impairment associated with pain. A typical list includes:
• Talks about pain.
• Moves in guarded fashion.
• Grimaces or rubs or touches a painful area.
• Reclines (or sits in a particular position) at a point in time when, were there no pain problem, it would not occur.
• Asks for medication or some other palliative procedure (heat pad, massage).
• Asks to be excused from or relieved of some activity because otherwise pain will occur or be aggravated.
The list may not include all of these, but most of them are common. The final list should probably have about five to ten items. More than that is excessively detailed. Items can be grouped into homogeneous clusters. Fewer than five or six items probably indicates lack of effective observations by the spouse, and further observations during subsequent visits should be required.
Counting Pain Behaviors
By negotiation with the spouse, a fixed amount of each spouse visit with the patient is committed during which pain behaviors will be covertly counted. A balance needs to be found. The time should be long enough to provide a reasonable behavior sample but not so long as to stretch beyond practical limits the spouse’s ability simultaneously to visit and to count. Experience indicates that a 20-minute counting period is usually adequate. A longer counting period is often superfluous and excessively burdensome. Shorter counting periods may lead to inadequate spouse vigilance or recognition of the importance of the task.
Doubt about the spouse’s readiness or ability to handle a 20-minute counting period may require a shorter interval initially. This can perhaps be increased at a later time when more mastery has been developed.
Counting periods should be constant in length, so for as possible, to permit meaningful comparisons across visits.
During each of the first several visits, the spouse is assigned the task of counting the number of times any one or combination of the pinpointed pain behaviors occur. It is not necessary, except in rare instances, to record the rate of each pain behavior separately, only the number of times anyone or more of them occur. At the end of the counting period, the spouse should be prepared to state with some precision how many pain behavior display events occurred. Moreover, the spouse should keep a record so that the number for each visit is retrievable. It should be made clear to the spouse that at the next session he or she will be expected to report specific numbers; for example, Tuesday evening, six; Wednesday evening, eight; Saturday afternoon, five.
The counting task can be made easier by pointing out to the spouse that a new pack of book matches provides a convenient counter. Each time a pain behavior is displayed, the spouse can bend a match from the book while it is held in a pocket or unobtrusively in the hand. It is a simple matter to count at the end of the visit how many matches have been bent.
The spouse should also record the count of verbal pain behaviors during the length of telephone conversations with the patient, and the records should note that it pertains to a telephone conversation. For lengthy telephone conversations, the same 20-minute limit can be used. For shorter calls, the compromise with necessity is to rely on the length of the call as a reasonable basis for an estimate.
More often than not, spouses will underestimate the counting task. At the time of the second session, the spouse will report that counting was forgotten or that “there were a lot of (or few) pain behaviors.” Additional counting sessions must be carried out until there is a consistent reporting of numerical values by the spouse. The numbers themselves need not be consistent, but the counting of them must be.
Keeping a covert count of one’s spouse’s behavior while also visiting with that spouse understandably can raise difficulties in interpersonal communication. In practice, this proves less of a problem than one might expect. In the first place, both patient and spouse will have been informed before treatment that there would be a training program for the spouse concerned with his or her reactions to pain and to activity. In addition, however, the issue of making a covert count of one’s mate’s behavior should be discussed explicitly with the spouse. There is no critical reason why the counting must be kept a secret. It should be emphasized that if the spouse wishes to tell his or her mate that the counting is going on, it is perfectly all right to do so. The telling will in no way obstruct the program. Once that is made clear, it can also be added that “it is usually easier in terms of your communication with your spouse that you say nothing about your counting. However, if for any reason you feel you should tell him/her, by all means do so. Otherwise, we recommend that you simply not discuss it until later in the program.” The handful of times in which the spouse has reported to the patient that he or she was counting did not lead to any untoward difficulties.
The function of the count is not to develop some form of quota. The baseline rate of pain behaviors displayed to the spouse can be used as a reference point against which the rate at later points in treatment can be compared. But that rarely proves necessary. The data are there, however, and should the spouse need special encouragement, later counts can be taken. The major reason for counting is that to do so forces increased vigilance. The reported count is a method for determining when the spouse has developed skill at discriminating pain behaviors from other ongoing patient behavior.

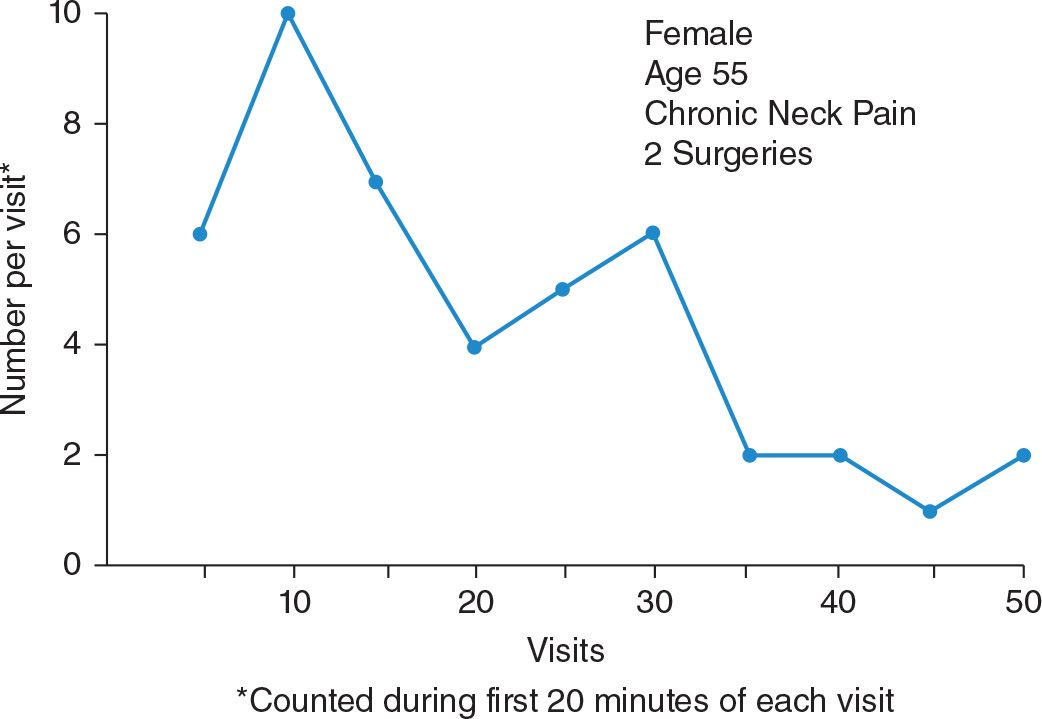
Figure 5 shows counts by a husband of his wife’s pain behaviors. Their home was several hundred miles away. The husband accompanied her to her admission. After a brief instructional session, he counted pain behaviors the first 20 minutes of a visit with her on the ward the second day of her treatment. He returned to his home and his work but again visited 2 weeks later and again counted. Between those visits he counted pain behaviors during telephone conversations with her. Those counts are shown in the upper part of the figure. This patient’s operant pain related in part to deprivation of reinforcers from her preoccupied husband. In later phases of treatment, when the husband appeared to have mastered discriminating pain behaviors and his own responses to them, the psychologist working with him in the retraining process assigned him the task of counting his reinforcers of his wife’s activity. For the first 20 minutes of each visit or telephone conversation, the husband counted the number of times he provided some word of praise, encouragement, or approval to his wife when she engaged in movement and activity. A sample of those counts is shown in the lower part of Figure 5.
Figure 6 portrays the trend of a patient’s pain behaviors observed and counted by his wife during the first 20 minutes of her numerous visits with him. In this particular case, the wife continued to count pain behaviors throughout the program because her efforts in his behalf seemed to realize considerable reinforcement from observing the continuing reduction in what had once been virtually incessant complaints of pain.
Pinpointing Spouse Responses
Once mastery of counting patient pain behavior has been demonstrated, it may be discontinued or held in abeyance to be resumed only if further need for it should arise. The next step is to train the spouse to identify his or her own responses to patient pain behavior and to patient activity.
The objective of this second step is to make it easier for the spouse to begin to change. What is to change first needs to be identified.
One procedure for the second step is to instruct the spouse to note precisely what he or she does in the first seconds after a display of pain behavior by the patient. The spouse can he instructed that during succeeding visits with the patient, for each of the first three pain behavior displays, the spouse is to make a mental note of exactly what he or she does. This instruction is often helped by the explanation, “It is as if we were going to videotape what you do while the patient is displaying pain. What would the tape show you doing, and what would we hear?”
A session with the spouse should be scheduled soon after the first attempts at self-observation to help firm up the efforts and to gain better recovery of the spouse’s recall. It usually takes several visits before mastery over this task emerges. As noted in the earlier discussion on patient evaluation, the spouse cannot do “nothing” in response to a pain display. “Nothing” takes many forms. A rather consistent pattern of spouse behaviors that follow pain displays usually emerges.
The self-observation task is difficult to do with precision. If the process is not moving ahead well, it is often useful to schedule a joint appointment of patient and spouse in which each tries to identify both his or her own and the mate’s responses. The patient develops a list of pain behaviors and another list of spouse reactions to them. The spouse develops a list of patient pain behaviors and of spouse reactions to them. These two pairs of lists can then be compared and discussed within the session. Such a session nearly always breaks the logjam and helps the spouse better to pinpoint.
The same sequence is followed in regard to the step of training spouse responses to patient exercise or activity. This step can sometimes be lumped with the second step, the work on the responses to pain behavior, and dealt with simultaneously. If that seems too difficult, they can be treated consecutively.
Withdrawing Attention to Pain Behavior
Consistency of spouse reports as to what he or she did after pain behavior and activity displays during visits with the patient is an indication of mastery over the self-observation pinpointing task. When that mastery has occurred, the next step is to examine the roster of spouse responses to pain behaviors, one by one, and to develop alternatives appropriate to treatment objectives. When the spouse has been discouraging patient exercise or activity, alternatives for those behaviors also need to be developed.
In the case of spouse reactions to pain behaviors, the major objective is to develop skill at being socially nonresponsive. Ways of doing this have already been discussed in relation to staff training. A simple and usually adequate remedy to the problem is to instruct the spouse, when pain behavior is seen or heard, to first break eye contact. Shifting one’s gaze from eye contact to the patient’s shoulder, for example, is a specific action, easily done, and easily remembered. The spouse can then be instructed to pause for a couple of seconds and then to ask the patient a question about some aspect of activity. The graphs displayed at the bedside offer a most convenient selection of topics or questions on which the spouse can draw.
Changing well-habituated ways of behaving after the occurrence of pain behavior is more easily described than accomplished. The task can be made easier by providing specific rehearsal sessions within the spouse training sessions. This kind of role playing helps the spouse have confidence and more precision.
Two or three visits during which these responses are rehearsed with the patient are usually required before moving on to the final step in the process.
Spouse Reinforcement of Activity and Well Behavior
The roster of ways in which a spouse has been discouraging activity is reviewed. The first change in that may simply be the admonishment not to do it, but that is rarely enough. The spouse’s task is made easier and the marital relationship is furthered if the spouse has a generally supportive response to offer at the appropriate moments.
A roster of ways to express support or approval is easily developed in a few moments of discussion, should that be needed. The task is to increase the use of these responses at the proper times. To accomplish that, the next spouse assignment can be to count the number of times that he or she reinforces the patient for activity or well behavior.
By the time this phase of training is reached, the patient will almost surely be ready for evening and weekend passes. As with the earlier counting of pain behavior by the spouse, counting periods can be set up. For an evening pass, it might be the first hour. For a 2-day weekend pass, it might be 30-minute counting periods during each morning, afternoon, and evening. During those counting periods, the spouse is instructed to count the number of times he or she reinforces the patient for activity. The only constraint is that reinforcement is not to occur contiguous to pain behavior. There should be ample opportunity for reinforcement, since the patient is bound to be doing something.
One might properly question whether a spouse will simply lavish arbitrary praise on the patient for doing essentially nothing, and thereby build up the count; for example, “It’s sure good to see you sitting there reading the newspaper,” said three times in 5 minutes. That kind of frivolous effort should, in the practical case, offer no hazards. Even a modicum of rapport with the spouse in the training sessions should be enough to avoid that kind of sloppy effort.
Spouse visits to and observations of physical therapy or other treatment sessions provide additional and convenient opportunity for rehearsal of the reinforcement of activity.
It is sometimes helpful to arrange for programmed mutual reinforcement of patient and spouse during the course of a pass or an evening recreation program. A spouse may have the mission of counting the number of times he or she reinforces the patient for activity. The patient may have the task of counting the number of times he or she receives reinforcement for activity. This mutual reinforcement can be done covertly or with mutual awareness that it is underway. Perhaps some will be surprised to observe that effectiveness rarely appears to be diminished by both parties being aware that the counting is going on.
There is no formal target number of reinforcements for activity to be attained. It becomes strictly a matter of judgment as to when the spouse has mastered adequately the task of avoiding pain-contingent social reinforcement and of providing sufficient intermittent reinforcement of suitable activity or well behavior.
Commentary: Pain Within a Social Context: Towards an Understanding of Bidirectional Influences
The key assertion developed in this chapter is the notion that others, in particular healthcare providers and spouses, may impact patient functioning by the attention they pay towards pain behaviors versus well behaviors. In this way, responses of others are considered as potential discriminative cues for pain behaviors or well behaviors within an operant approach to pain. These ideas have had a substantial impact upon theory as well as clinical practice of pain. First, since the publication of Fordyce’s book in 1976, it has been well accepted that psychosocial treatment of chronic pain should focus upon restoration of function rather than on pain reduction per se. Second, Fordyce’s description of the social-contextual factors impacting pain in 1976 stimulated research on the social dimensions of pain and pain expression. At present, it is widely acknowledged that pain is not only a personal experience but takes place within a social context [38].
THE ROLE OF OTHERS AS DISCRIMINATIVE CUES OF PAIN EXPRESSION
In the last decades, numerous experimental and clinical studies have been published demonstrating the importance of social-contextual variables in pain. In particular, evidence shows that pain behaviors may be operantly controlled by verbal reinforcement (e.g., [41]) and that others may act as discriminative cues of pain expression (see [48]). Notably, children as young as nine years report showing less pain in presence of a peer than when with their parent [89]. The most important reason for hiding their pain, as reported in this study by Zeman & Garber [89], was the expectation of negative interpersonal consequences.
In his review, Krahe et al. [48] identified that pain (expression) is influenced by (a) the pre-existing relationship with the other person present (e.g., acquaintance versus stranger), (b) the degree to which individuals can perceive the intentions of the other person, (c) the degree to which the other is perceived as having the possibility to act, and (d) individual differences in relating to others (e.g., attachment style) and coping with pain. Regarding the latter, the interaction between children’s beliefs about pain and social-contextual variables has been investigated in our lab [76–80]. An interesting finding from our studies is that children who perceive their pain as threatening (i.e., catastrophize about pain) display facial pain behaviors, regardless whether they are alone, in the presence of a stranger or a parent. In contrast, the facial display of children perceiving pain as non-threatening (i.e., low catastrophizers) was shown to be much more dependent upon the context. Specifically, low catastrophizing children displayed more facial pain behaviors in the presence of a parent than when alone or in presence of a stranger [76,79]. In contrast to children, contextual variables impact the modulation of pain expression by high catastrophizing adults. A study by Sullivan and colleagues [68] showed that high catastrophizing undergraduates, requested to immerse their arm in a cold water box, displayed communicative pain behaviors (e.g., facial pain expression) for a longer duration when they were in the presence of an observer (i.e., a research assistant) than when being alone.
SOLICITOUS SPOUSE AND PARENT RESPONSES
A number of studies have been published investigating the impact of solicitous spouse and parent behaviors upon individual’s (clinical) pain outcomes. Solicitous behaviors have been defined as “Statements inquiring about or exhibiting concern for the other’s physical condition or comfort; offers of assistance; behavior discouraging the other from activity; physical assistance or taking over a task” (p. 779; [64])” and have been conceptualized as reinforcing patients’ pain behaviors. The impact of solicitous responses has been investigated most often using questionnaires. The most frequently used questionnaires in adult populations are the West Haven-Yale Multidimensional Pain Inventory (WHYMPI; [46]) and the Spouse Response Inventory (SRI; [66]), while in pediatric populations, a wider range of questionnaires has been employed. These include the Illness Behavior Encouragement Scales (IBES; [83]), the Social Consequences of Pain Questionnaire (SCP; [82]), the Adult Responses to Children’s Symptoms Questionnaire (ARCS; [72]), the Pain-related Parent Behavior Inventory (PPBI; [39]), and the Inventory of Parent/Caregiver Responses to the Children’s Pain Experience (IRPEDNA; [40]).
In the context of adult pain, evidence (see [59]) shows that patients whose spouses more frequently engage in solicitous behavior tend to report or exhibit higher levels of pain behavior [64,65,71], more disability and dysfunction [25,62,71], and use higher doses of opioids [17]. In contrast, partner encouragement of patient well behaviors has been related to lower levels of patient-reported pain behavior [17]. These research findings are corroborated in the context of pediatric pain. Generally, solicitous or so-called protective behaviors in parents have been found to be associated with worse child outcomes (for an overview, see [32]). Across studies, parental protective behaviors have been related to higher child functional disability [51,61,67] and worse school functioning [42,56]. Furthermore, studies have shown that parental protective behaviors may negatively impact child functioning through their effects upon child fear-avoidance beliefs [37,87]. Through their protective behaviors, parents may fuel fearful appraisals of pain in their child, which may motivate children to avoid activities, resulting in disability [32].
Interestingly, recent studies have focused on the identification of factors that predispose parents to engage in (persistent) solicitous or protective behaviors. An important variable that has been identified is the presence of catastrophizing thoughts about the child’s pain (i.e., a parent’s tendency to focus on and exaggerate the threat value of the child’s pain and to negatively evaluate his/her ability to deal with the child’s pain) [31]. Research findings support a cognitive-affective model of pain: parents who endorse high levels of catastrophizing thoughts about their child’s pain often experience high distress, which may motivate them to engage in behaviors aimed at the reduction or avoidance of pain in their child [32]. Studies have shown that high levels of parental catastrophizing are related to high levels of parental distress [4,6,31,36], a high priority to engage in (persistent) attempts at controlling the child’s pain [5], and a strong tendency to restrict their child’s activities [6,35]. Furthermore, protective behaviors have been demonstrated to explain the association between parental catastrophizing and child outcomes, such as school impairment and functional disability [56,67].
OPERANT TREATMENT
Since 1976, numerous studies have examined the effectiveness of an operant approach to the psychosocial treatment of chronic pain. In general, behavioral treatment of patients with chronic low back pain has been shown to be effective in reducing pain intensity, increasing activity levels, improving functioning, and in decreasing medication use [26,63,73]. The effects are, however, only small to moderate [73]. With regard to spousal involvement in therapy, evidence is available that time-contingent spouse reinforcement of increased activity levels and decreased medication intake leads to positive outcomes, while pain-contingent spouse reinforcement of decreased activity and increased medication intake is related to poor outcomes (see [63]).
Furthermore, research shows that treatment results improve when other treatment approaches are added to operant treatment. In a study by Vlaeyen and colleagues [81], patients were assigned to one of three treatment conditions: 1) operant treatment alone, 2) operant treatment combined with cognitive treatment (aimed at decreasing catastrophizing pain cognitions and at increasing self-efficacy expectations), or 3) operant treatment combined with respondent treatment (aimed at decreasing muscle tension levels in response to tension-eliciting situations, by means of relaxation techniques, EMG-biofeedback and exposure). The study demonstrated that treatments involving both operant and respondent treatment and cognitive treatment modules were more efficacious than operant treatment alone. The addition of respondent or cognitive treatment modules was found to reduce patients’ catastrophizing thoughts about pain in the long term, a variable which has been shown to play a major role in the development and maintenance of chronic pain problems [52].
CRITICAL REFLECTIONS AND RECENT DEVELOPMENTS
Although the merits of the operant conceptualisation of pain are beyond doubt, several critical reflections have been formulated in the last decade. Below I outline briefly the main further developments in theory and clinical practice regarding the role of the social context, which have advanced and elaborated the operant approach to pain and functioning.
A main criticism of the operant model, and in particular the role of social attention in the reinforcement of pain behaviour, has been the overall oversimplification and the neglect of the complex processes involved in interactions between patients and others (e.g., spouses) [9,26,59]. The growth of studies in the last decades, in different scientific domains including clinical health psychology, evolutionary psychology and behavioural neuroscience, provides evidence for the complexity of interactions between individuals in pain and their immediate environment (for an overview see [38]). As indicated by the communications model of pain [38], understanding the complex interactions between a pain sufferer and his/her social context requires understanding of (1) why and how pain experience becomes manifest in behaviour, (2) how and why others attend to, interpret, and respond to specific cues presented by the person in pain, and (3) how others, in turn, impact upon the patient’s future pain experience, pain behaviour, and functioning [29,30,33].
Facial Expressions of Pain
First, it has been argued that the facial display of pain is not (only) shaped by social reinforcement as stated in operant learning theory, but evolutionarily hardwired. In her seminal paper published in 2002, Williams [86] argued that the facial expression of pain has an innate communicative function, aiming to solicit help from others. However, when growing up people learn to (partially) suppress and control the facial display of pain in particular situations. For example, it has been suggested that individuals experiencing pain may hide their pain to avoid negative reactions in case of social threat [60], to avoid upsetting others [16], or to preserve relationship harmony [9].
Empathy
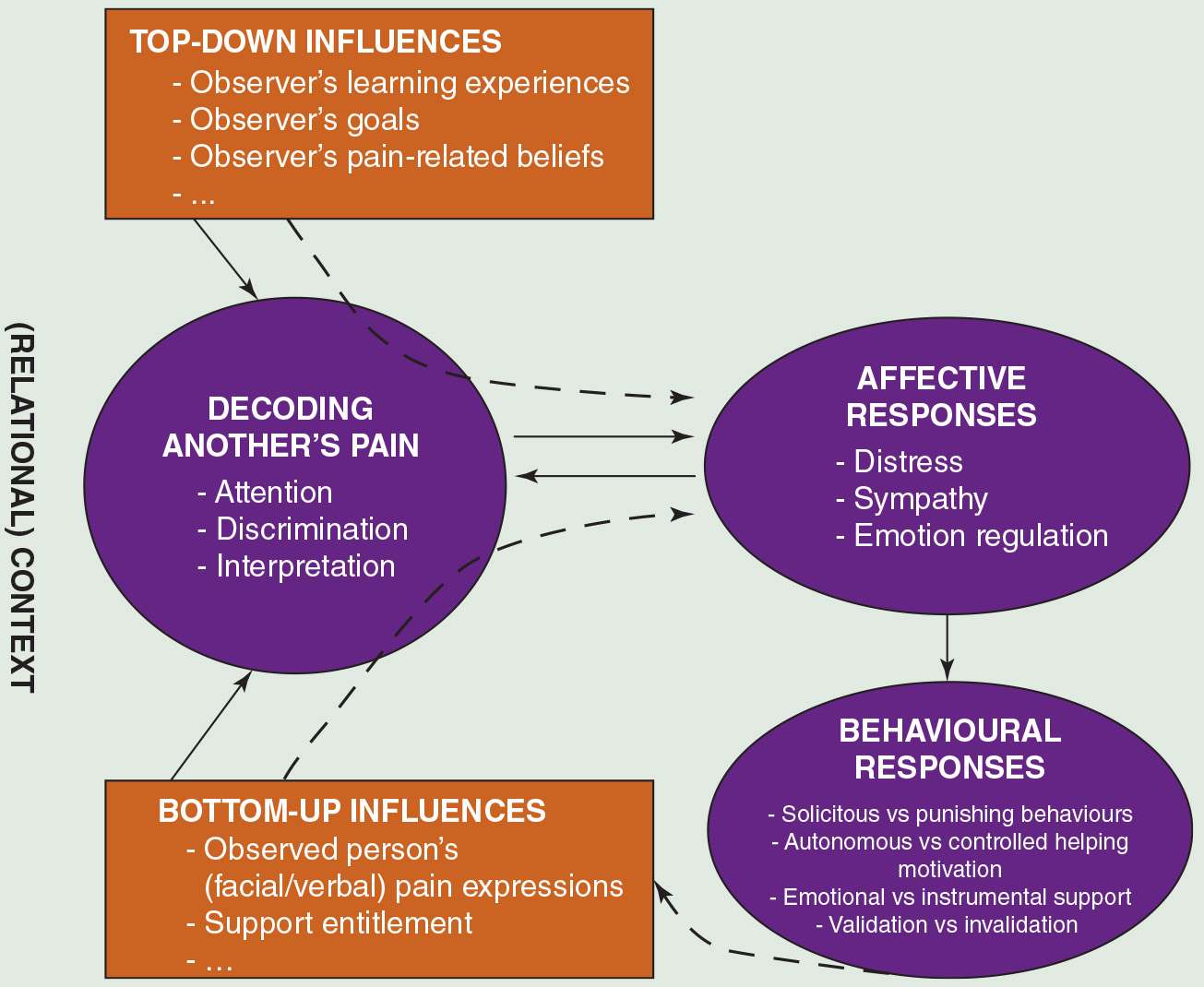
Second, an important area neglected in a purely operant perspective is the effects of observing pain upon others (e.g., spouses) themselves. This was depicted in a model of empathy in the context of pain, outlined in 2005. This model advanced the field by proposing that characteristics of the individual in pain (“bottom-up”; e.g., pain expression) and observer characteristics (“top-down”; e.g., trait anxiety) may impact cognitive, affective and behavioural responses of others in the immediate environment, which in turn may impact individual’s pain and pain expression ([30,33]; see Figure 1). Research has shown that observing others in pain induces distress [3,7], particularly when pain is perceived as highly threatening [7,31]. Research further shows that spouses of chronic pain patients often experience declines in psychological well-being and relationship satisfaction [10,24,27,53]. These, in turn, may impact their behaviours towards the patient, and as such, patient outcomes. For instance, an observational study in 95 chronic pain couples [14] showed that higher levels of spousal anxiety were associated with invalidating spouse behaviours (i.e., behaviours expressing contempt, disrespect and/or nonacceptance of patient’s disclosures of pain and distress). Empathy models would predict that experiencing personal distress when observing someone else’s pain might induce a self-oriented focus inhibiting the ability to attend to the other person’s needs [30,33,34]. An alternative explanation proposed by Cano and colleagues [14] is that distressed spouses intentionally respond with invalidation in an attempt to reduce their partner’s distress, and as such, their own distress. Future research is needed to further disentangle why partners of chronic pain patients are distressed, and how this may impact their behavioural responses. Thus, not only observers’ characteristics (e.g., catastrophizing thoughts about patient’s pain) may impact others’ distress and support behaviours [12,53], but patient variables such as the patients’ level of catastrophizing about pain [8], patients’ perceived entitlement to support [13] and patients’ gratitude for the received help or support also may play a role (see [28,50]).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


